Department of Cardiothoracic Surgery, Jena University Hospital, Friedrich-Schiller-University, University of Jena, Am Klinikum 1, 07747, Jena, Germany.
Division of Cardiothoracic Surgery, University of North Carolina, Chapel Hill, USA.
BMC Cardiovasc Disord. 2024 Oct 21;24(1):580. doi: 10.1186/s12872-024-04252-9.
Liver dysfunction is a known risk factor in the cardiovascular field. It specifically increases perioperative risk in patients undergoing coronary bypass surgery. Since percutaneous coronary intervention (PCI) is the much less invasive procedure for the treatment of coronary artery disease, we aimed to assess the relationship of liver dysfunction with outcomes in patients undergoing PCI.
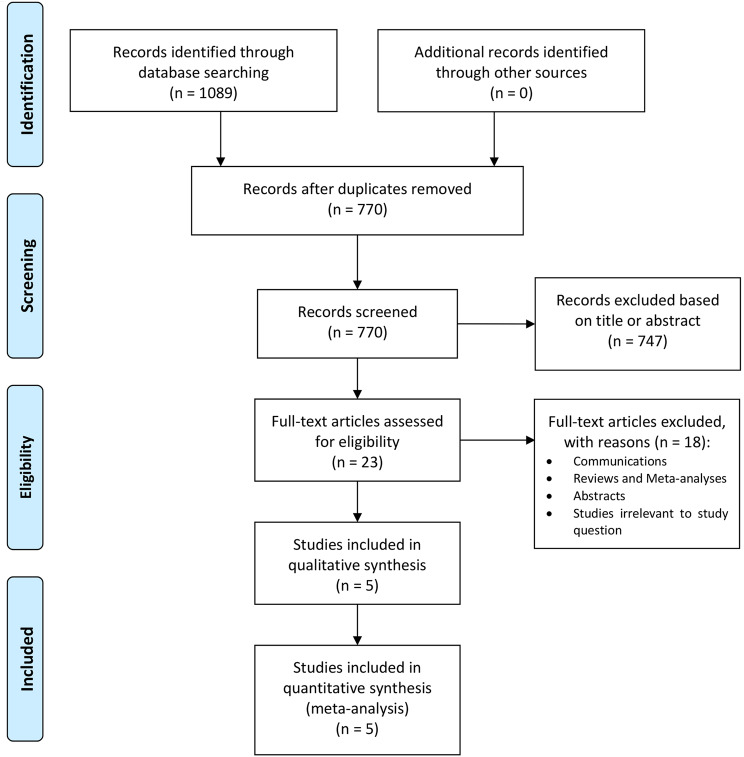
Three libraries were searched (MEDLINE, Web of Science and The Cochrane Library). We performed a meta-analysis of all studies in patients who underwent PCI that provided information on the presence or absence of liver dysfunction. Primary outcome was short-term mortality. Secondary outcomes were major adverse cardio- and cerebrovascular events (MACCE), bleeding and acute kidney injury. Random-effects model was applied.
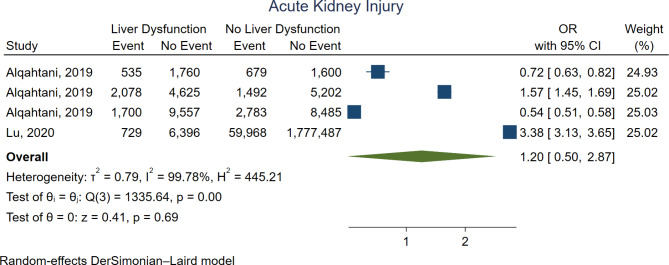
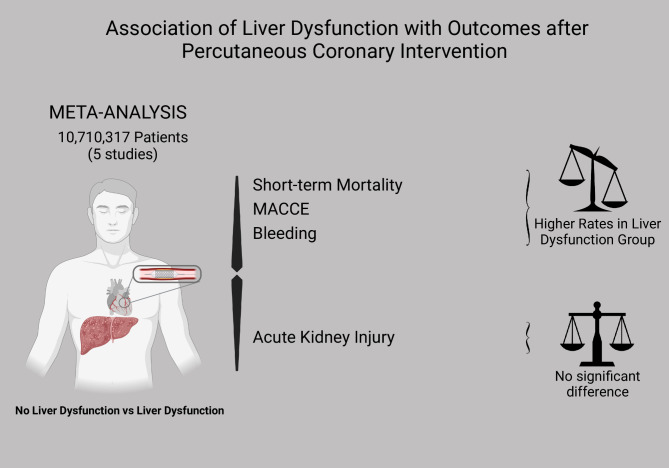
Five studies were selected and the data from 10,710,317 patients were included in the final analysis. In comparison with the absence of liver dysfunction, patients with liver dysfunction were associated with higher short-term mortality (OR 2.97, 95%CI 1.23-7.18, p = 0.02), higher MACCE (OR 1.42, 95%CI 1.08-1.87, p = 0.01), and higher bleeding (OR 2.23, 95%CI 1.65-3.00, p < 0.01). There was no significant difference regarding acute kidney injury (OR 1.20, 95%CI 0.50-2.87, p = 0.69).
The analysis suggests that liver dysfunction in patients undergoing PCI is independently associated with higher risk of short-term mortality and increased occurrence of MACCE and bleeding. However, there appears to be no association to acute kidney injury.
肝功能障碍是心血管领域的已知风险因素。它特别增加了接受冠状动脉旁路手术的患者的围手术期风险。由于经皮冠状动脉介入治疗(PCI)是治疗冠状动脉疾病的侵入性较小的手术,因此我们旨在评估肝功能障碍与接受 PCI 治疗的患者结局之间的关系。
搜索了三个数据库(MEDLINE、Web of Science 和 The Cochrane Library)。我们对所有提供有关肝功能障碍存在或不存在的接受 PCI 的患者的研究进行了荟萃分析。主要结局是短期死亡率。次要结局是主要不良心脑血管事件(MACCE)、出血和急性肾损伤。应用随机效应模型。
选择了五项研究,最终分析纳入了来自 10,710,317 名患者的数据。与无肝功能障碍相比,肝功能障碍患者的短期死亡率更高(OR 2.97,95%CI 1.23-7.18,p=0.02),MACCE 发生率更高(OR 1.42,95%CI 1.08-1.87,p=0.01),出血发生率更高(OR 2.23,95%CI 1.65-3.00,p<0.01)。急性肾损伤方面无显著差异(OR 1.20,95%CI 0.50-2.87,p=0.69)。
分析表明,接受 PCI 的患者的肝功能障碍与短期死亡率升高和 MACCE 及出血发生率增加独立相关。然而,与急性肾损伤似乎没有关联。