Department of Cardiothoracic Surgery, Friedrich-Schiller-University Jena, 101 Erlanger Allee, 07747, Jena, Germany.
Department of Cardiothoracic Surgery at New York Presbyterian, Weill Cornell Medical Center, New York, USA.
Sci Rep. 2022 Mar 24;12(1):5138. doi: 10.1038/s41598-022-09158-0.
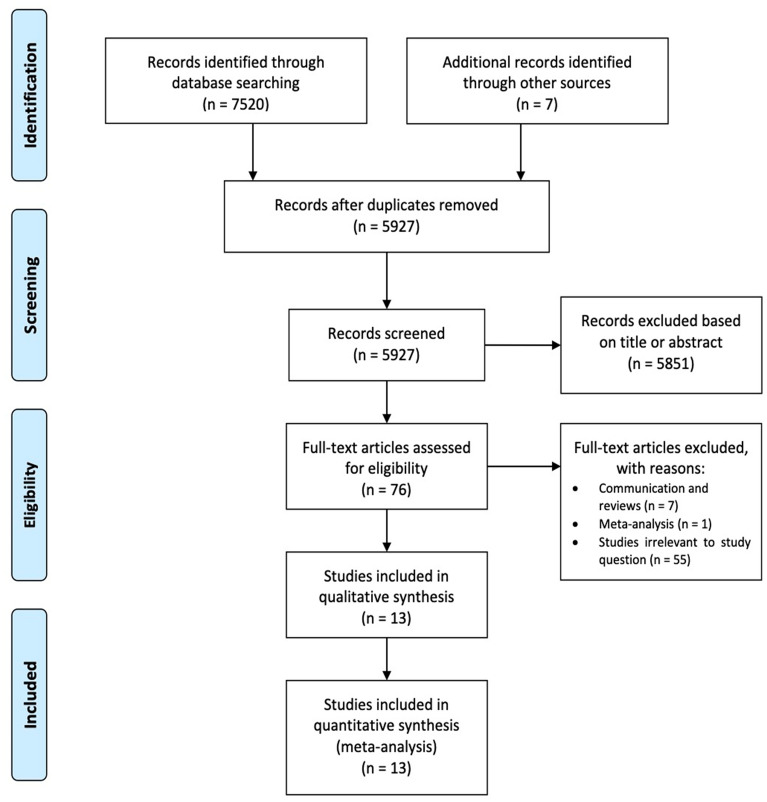
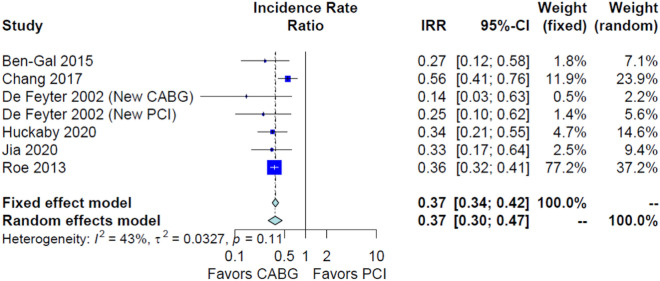
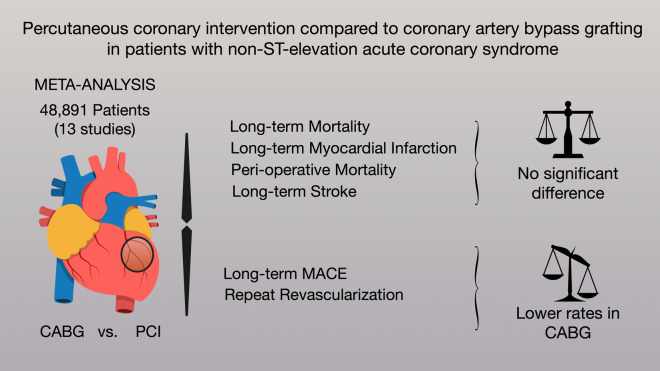
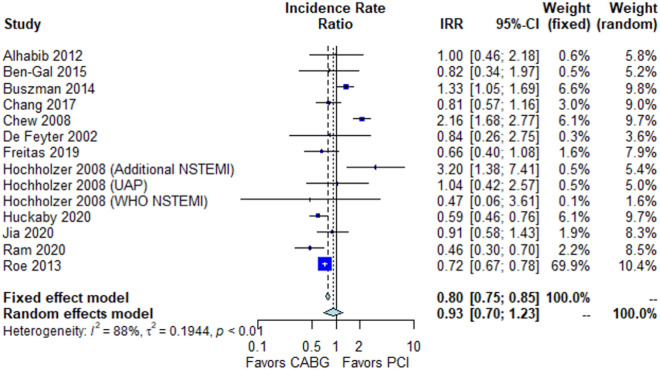
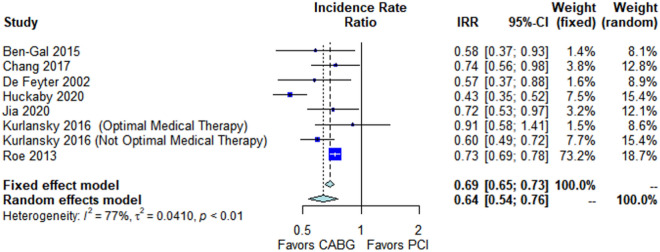
Non-ST-elevation acute coronary syndrome (NSTE-ACS) affects millions of patients. Although an invasive strategy can improve survival, the optimal treatment [i.e., percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG)] is not clear. We performed a meta-analysis of studies reporting outcomes between PCI and CABG in patients with NSTE-ACS. MEDLINE, EMBASE and Cochrane Library were assessed. The primary outcome was long-term mortality. Inverse variance method and random model were performed. We identified 13 observational studies (48,891 patients). No significant difference was found in the primary endpoint [CABG vs. PCI, incidence rate ratio (IRR) 0.93, 95% confidence interval (CI) 0.70; 1.23]. CABG was associated with lower long-term major adverse cardiovascular events (MACE) (IRR 0.64, 95% CI 0.54; 0.76) and lower long-term re-revascularization (IRR 0.37, 95% CI 0.30; 0.47). There was no significant difference in long-term myocardial infarction (CABG vs. PCI, IRR 0.96, 95% CI 0.50; 1.84) and peri-operative mortality (CABG vs. PCI, odds ratio 1.36, 95% CI 0.94; 1.95). For the treatment of NSTE-ACS, CABG and PCI are associated with similar rates of long-term mortality and myocardial infarction. CABG is associated with lower rates of long-term MACE and re-revascularization. Randomized comparisons in this setting are necessary.
非 ST 段抬高型急性冠状动脉综合征(NSTE-ACS)影响着数以百万计的患者。尽管侵入性策略可以提高生存率,但最佳治疗方法(即经皮冠状动脉介入治疗(PCI)或冠状动脉旁路移植术(CABG))尚不清楚。我们对报道 NSTE-ACS 患者 PCI 和 CABG 之间结局的研究进行了荟萃分析。评估了 MEDLINE、EMBASE 和 Cochrane 图书馆。主要结局是长期死亡率。采用逆方差法和随机模型进行分析。我们确定了 13 项观察性研究(48891 名患者)。主要终点无显著差异[CABG 与 PCI 相比,发生率比(IRR)为 0.93,95%置信区间(CI)为 0.70;1.23]。CABG 与较低的长期主要不良心血管事件(MACE)发生率相关(IRR 为 0.64,95%CI 为 0.54;0.76)和较低的长期再血管化发生率相关(IRR 为 0.37,95%CI 为 0.30;0.47)。长期心肌梗死(CABG 与 PCI 相比,IRR 为 0.96,95%CI 为 0.50;1.84)和围手术期死亡率(CABG 与 PCI 相比,优势比 1.36,95%CI 为 0.94;1.95)无显著差异。对于 NSTE-ACS 的治疗,CABG 和 PCI 与相似的长期死亡率和心肌梗死发生率相关。CABG 与较低的长期 MACE 和再血管化发生率相关。在这种情况下,需要进行随机对照比较。