Clinic for Paediatric and Adolescent Rheumatology, St. Josef-Stift Hospital, Northwest German Center for Rheumatology, Sendenhorst, Germany.
University of Halle-Wittenberg, Halle, Germany.
Pediatr Rheumatol Online J. 2024 Oct 21;22(1):94. doi: 10.1186/s12969-024-01029-4.
To identify an optimal pediatric musculoskeletal ultrasound (MSUS) protocol for the detection of knee arthritis in patients with juvenile idiopathic arthritis (JIA) including a comparison with existing protocols. Secondary aims were to correlate MSUS-identified B-Mode (BM) and Power Doppler-Mode (PD) synovitis with clinical findings.
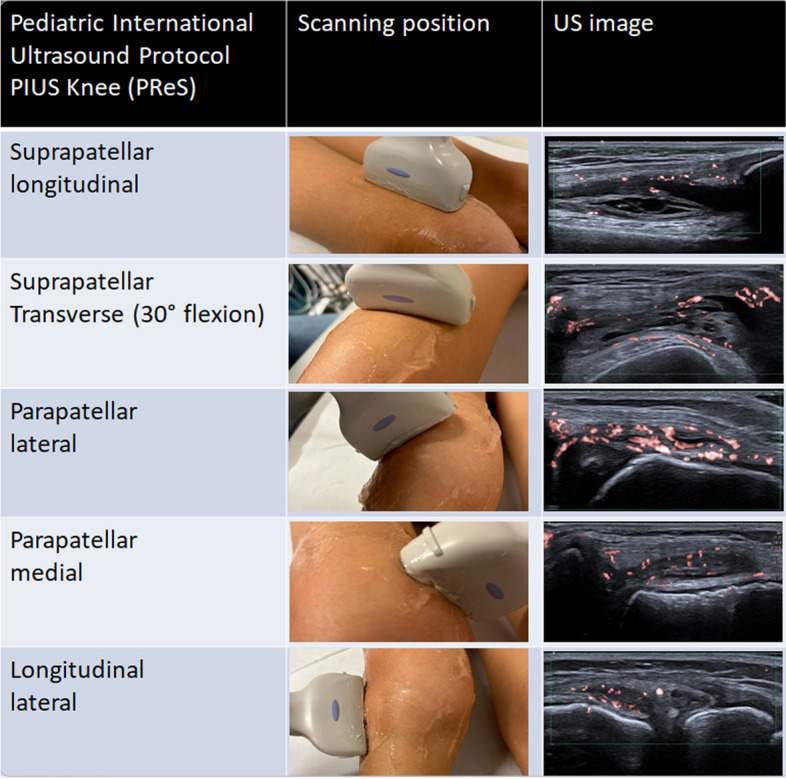
Consecutive JIA patients with confirmed knee arthritis after clinical examination underwent a thorough MSUS study protocol which included views identified and consented by the Pediatric Rheumatology european Society (PReS) Imaging Working Party for the detection of synovitis. In total eight views including measurement of the suprapatellar recess were included. Scoring of synovitis followed the pediatric OMERACT criteria (BM and PD severity grading 0 to 3). Interobserver reliability of BM and PD was tested before study begin. Previously published MSUS protocols for knee synovitis were also identified from the literature and their scan protocols compared to identify differences in sensitivity for synovitis according to the number and specific type of views included. Finally, a clinically applicable MSUS protocol for knee synovitis could be proposed.
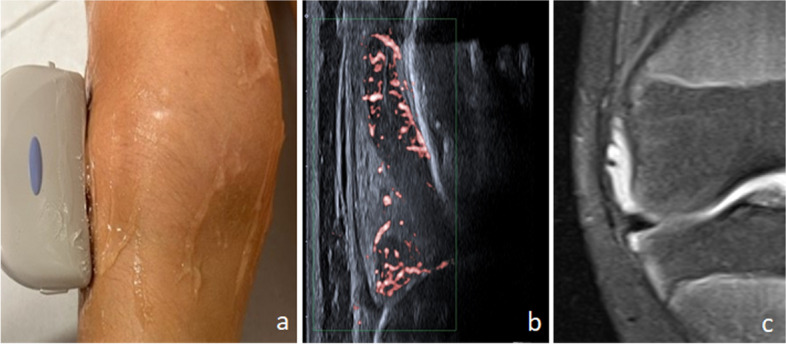
In 114 patients with clinically active knee inflammation, BM positivity (grading ≥ 1) was most frequently detected in the suprapatellar longitudinal and transverse scans performed in any positioning (frequency 97-99% in suprapatellar longitudinal in 30° or neutral respectively). PD positivity was however higher in these views performed in 30° flexion compared to neutral. Intrasynovial PD positivity (grading ≥ 1) was most frequently detected in the lateral parapatellar (69%, sensitivity 0.68, specificity 0.98), medial parapatellar (frequency 67%, sensitivity 0.67, specificity 1.0), the longitudinal lateral (68%, sensitivity 0.67, specificity 0.98) and suprapatellar transverse in 30° (frequency 64%, sensitivity 0.64, specificity 1.0). A combination of five views was the most sensitive for BM and PD synovitis. The suprapatellar recess size was analyzed by age and gender. For each group, the recess was wider in knees with arthritis than without (p < 0.001). Interobserver reliability of BM and PD positivity showed 85% agreement, with kappa 0.74 (very good). Three published studies with knee synovitis MSUS protocols were identified, which included a range of 1-3 views. Evaluation of the sensitivity of positive PD findings of each of these protocols reached a range of 53-83%; the highest sensitivity (91%) was achieved with the 5 views as identified by this study. These five views were therefore combined to form the Pediatric Internationally agreed Ultrasound (PIUS) knee protocol.
BM and PD positivity reliably correlated with the identification of pathological findings in knees of patients with JIA. From an internationally agreed protocol of eight images, a combination of five showed the greatest sensitivity for synovitis. This protocol, termed 'PIUS-Knee' performed well when compared to existing protocols.
确定一种最佳的儿科肌肉骨骼超声(MSUS)方案,用于检测幼年特发性关节炎(JIA)患者的膝关节关节炎,包括与现有方案的比较。次要目的是将 MSUS 识别的 B 模式(BM)和功率多普勒模式(PD)滑膜炎与临床发现相关联。
经临床检查确诊为膝关节关节炎的连续 JIA 患者接受了全面的 MSUS 研究方案,该方案包括由儿科风湿病欧洲学会(PReS)成像工作组确定并同意的用于检测滑膜炎的视图。总共包括 8 个视图,包括髌上隐窝的测量。滑膜炎的评分遵循儿科 OMERACT 标准(BM 和 PD 严重程度分级 0 至 3)。在研究开始前测试了 BM 和 PD 的观察者间可靠性。还从文献中确定了先前发表的用于膝关节滑膜炎的 MSUS 方案,并比较了它们的扫描方案,以根据包括的视图数量和特定类型来确定滑膜炎的敏感性差异。最后,可以提出一种临床适用的膝关节滑膜炎 MSUS 方案。
在 114 名患有临床活动性膝关节炎症的患者中,BM 阳性(分级≥1)最常出现在任何位置进行的髌上纵向和横向扫描中(在 30°或中立位时髌上纵向的频率为 97-99%)。然而,在 30°弯曲位进行的这些视图中,PD 阳性率更高。关节内 PD 阳性(分级≥1)最常出现在外侧髌旁(69%,敏感性 0.68,特异性 0.98)、内侧髌旁(频率 67%,敏感性 0.67,特异性 1.0)、外侧髌旁(68%,敏感性 0.67,特异性 0.98)和髌上横向 30°(频率 64%,敏感性 0.64,特异性 1.0)。五种视图的组合对 BM 和 PD 滑膜炎最敏感。髌上隐窝的大小通过年龄和性别进行了分析。对于每组,关节炎膝关节的隐窝宽度均大于无关节炎膝关节(p<0.001)。BM 和 PD 阳性的观察者间可靠性显示 85%的一致性,kappa 值为 0.74(非常好)。确定了三种具有膝关节滑膜炎 MSUS 方案的已发表研究,其中包括 1-3 个视图。对这些方案中每个方案的阳性 PD 发现的敏感性评估范围为 53-83%;本研究确定的 5 个视图的敏感性最高(91%)。因此,这 5 个视图被组合形成儿科国际协议超声(PIUS)膝关节方案。
BM 和 PD 阳性与 JIA 患者膝关节病理发现的识别可靠相关。从国际协议的 8 个图像中,组合 5 个显示出对滑膜炎的最大敏感性。与现有方案相比,该方案称为“PIUS-膝关节”,表现良好。