Algeri L, Falkman L, Spada F, Frassoni S, Bagnardi V, Boselli S, Cardinale D, Zanobini M, Crona J, Benini L, Tamayo D, Mazzon C, Gervaso L, Cella C A, Zampino M G, Ciardiello D, Russo A, Badalamenti G, Welin S, Fazio N
Division of Gastrointestinal Medical Oncology and Neuroendocrine Tumors, European Institute of Oncology (IEO), IRCCS, Milan; Department of Precision Medicine in Medical, Surgical and Critical Care (Me.Pre.C.C.), Section of Medical Oncology, University of Palermo, Palermo, Italy.
Department of Endocrine Oncology, Uppsala University Hospital, Uppsala, Sweden.
ESMO Open. 2024 Nov;9(11):103959. doi: 10.1016/j.esmoop.2024.103959. Epub 2024 Oct 22.
Up to 50% of patients with advanced small-intestinal neuroendocrine tumors (SI-NETs) and carcinoid syndrome (CS) develop carcinoid heart disease (CHD). However, the true frequency and prognostic markers for CHD in CS are lacking. We described the real-world management of patients in two NET referral centers in this clinical context and relationships between clinical features, including CHD and overall survival (OS).
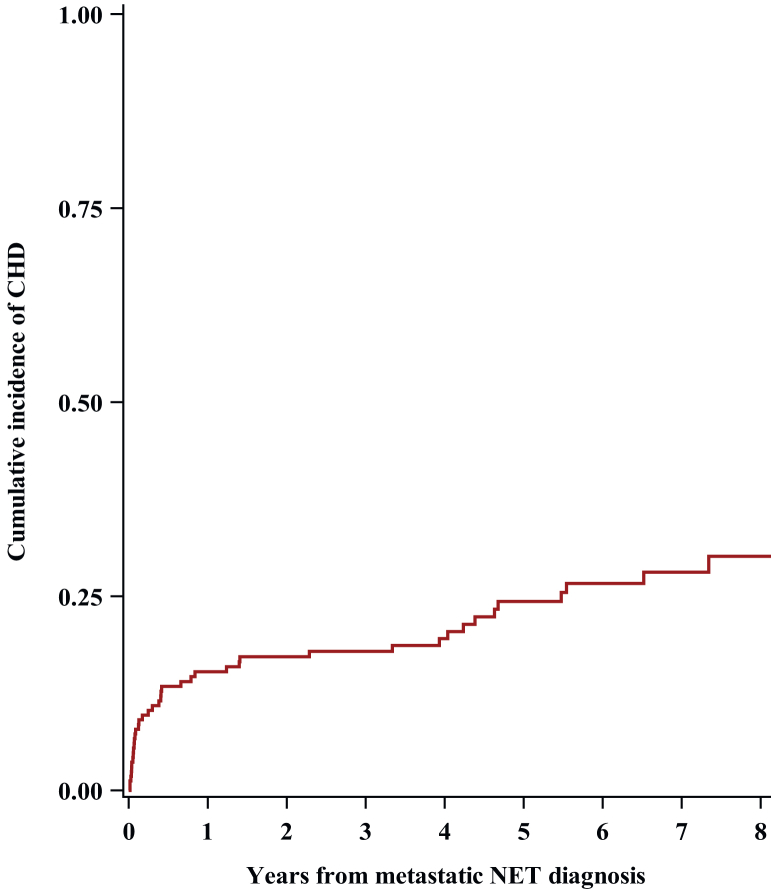
This is a retrospective analysis of patients with stage IV SI-NET and CS, treated at the European Institute of Oncology in Milan and Uppsala University in Sweden between 2015 and 2021. CHD was defined as at least one moderate right-sided heart valve defect. Median OS and cumulative incidence of CHD were estimated from the diagnosis of metastatic disease, and the association between clinical parameters with both OS and occurrence of CHD was evaluated.
We included 165 patients, with 97% having low-intermediate-grade SI-NETs and 86% having synchronous liver metastases. Ninety-eight patients (59%) became refractory to full label dose of somatostatin analogues and 25% developed a CHD. At CHD diagnosis, baseline urine 5-hydroxyindoleacetic acid (24-h u5-HIAA) value and plasma N-terminal pro-brain natriuretic peptide (NT-proBNP) value were known in 76% of patients. Moderate-to-severe tricuspid insufficiency was the most common alteration of CHD. Prognosis was significantly impaired by CHD (multivariable hazard ratio for OS = 2.85, P < 0.001). The median OS from the CHD diagnosis was 4.5 years [95% confidence interval (CI) 2.1-7.2 years], and the 5-year survival rate was 34% (95% CI 13% to 57%).
In our study population of SI-NET patients with CS, more than half had a refractory carcinoid syndrome (RCS) and one-quarter developed a CHD, with a negative impact on OS. Therefore, it is recommended to screen and monitor patients with CS for CHD, ideally with a combination of u5-HIAA, NT-proBNP values, and echocardiography at CS baseline, preferably in NET referral centers.
高达50%的晚期小肠神经内分泌肿瘤(SI-NETs)和类癌综合征(CS)患者会发生类癌性心脏病(CHD)。然而,CS中CHD的真实发生率和预后标志物尚不清楚。我们描述了在此临床背景下两个NET转诊中心患者的实际管理情况,以及包括CHD和总生存期(OS)在内的临床特征之间的关系。
这是一项对2015年至2021年期间在米兰的欧洲肿瘤研究所和瑞典的乌普萨拉大学接受治疗的IV期SI-NET和CS患者的回顾性分析。CHD被定义为至少有一个中度右侧心脏瓣膜缺损。从转移性疾病诊断开始估计CHD的中位OS和累积发生率,并评估临床参数与OS和CHD发生之间的关联。
我们纳入了165例患者,其中97%患有低中级SI-NETs,86%有同步肝转移。98例患者(59%)对全量生长抑素类似物治疗无效,25%发生了CHD。在CHD诊断时,76%的患者已知基线尿5-羟吲哚乙酸(24小时u5-HIAA)值和血浆N末端脑钠肽前体(NT-proBNP)值。中重度三尖瓣关闭不全是CHD最常见的改变。CHD显著损害了预后(OS的多变量风险比=2.85,P<0.001)。从CHD诊断开始的中位OS为4.5年[95%置信区间(CI)2.1 -