Cardiovascular Disease Program, Monash Biomedicine Discovery Institute, Monash University, Clayton, VIC, 3800, Australia.
Department of Pharmacology, Monash University, Clayton, VIC, 3800, Australia.
Stem Cell Res Ther. 2024 Oct 23;15(1):375. doi: 10.1186/s13287-024-03992-x.
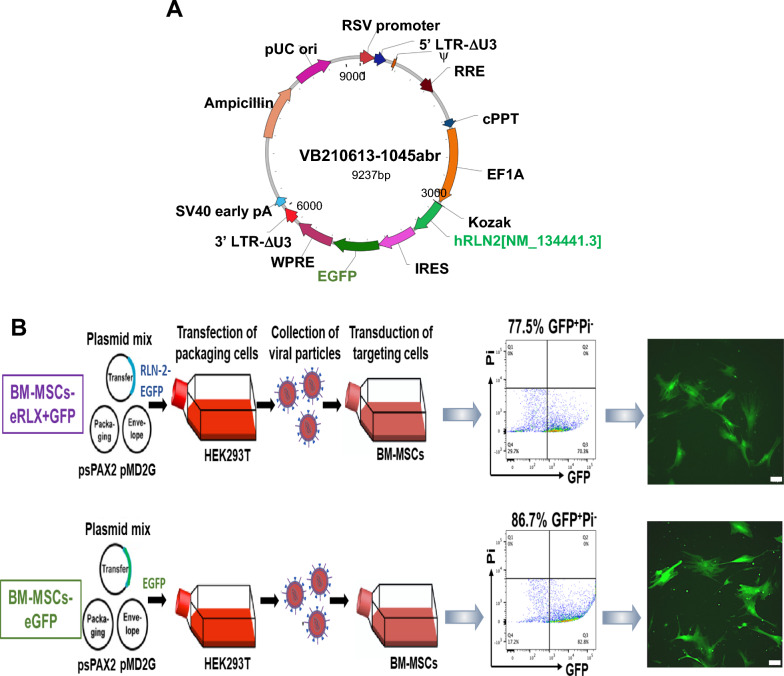
Kidney fibrosis is a hallmark of chronic kidney disease (CKD) and compromises the viability of transplanted human bone marrow-derived mesenchymal stromal cells (BM-MSCs). Hence, BM-MSCs were genetically-engineered to express the anti-fibrotic and renoprotective hormone, human relaxin-2 (RLX) and green fluorescent protein (BM-MSCs-eRLX + GFP), which enabled BM-MSCs-eRLX + GFP delivery via a single intravenous injection.
BM-MSCs were lentiviral-transduced with human relaxin-2 cDNA and GFP, under a eukaryotic translation elongation factor-1α promoter (BM-MSCs-eRLX + GFP) or GFP alone (BM-MSCs-eGFP). The ability of BM-MSCs-eRLX + GFP to differentiate, proliferate, migrate, produce RLX and cytokines was evaluated in vitro, whilst BM-MSC-eRLX + GFP vs BM-MSCs-eGFP homing to the injured kidney and renoprotective effects were evaluated in preclinical models of ischemia reperfusion injury (IRI) and high salt (HS)-induced hypertensive CKD in vivo. The long-term safety of BM-MSCs-RLX + GFP was also determined 9-months after treatment cessation in vivo.
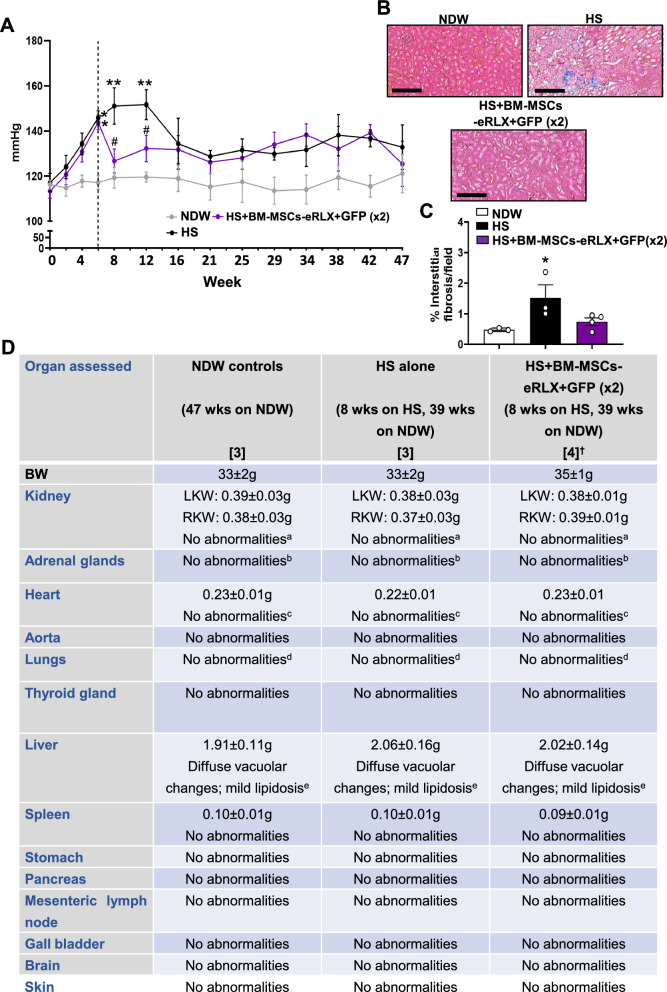
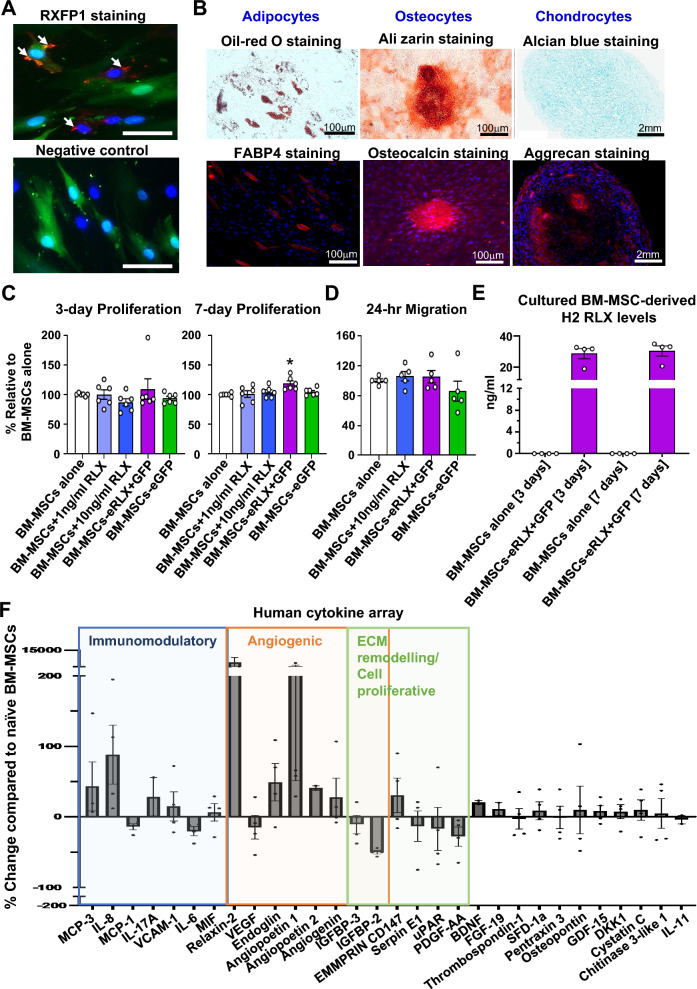
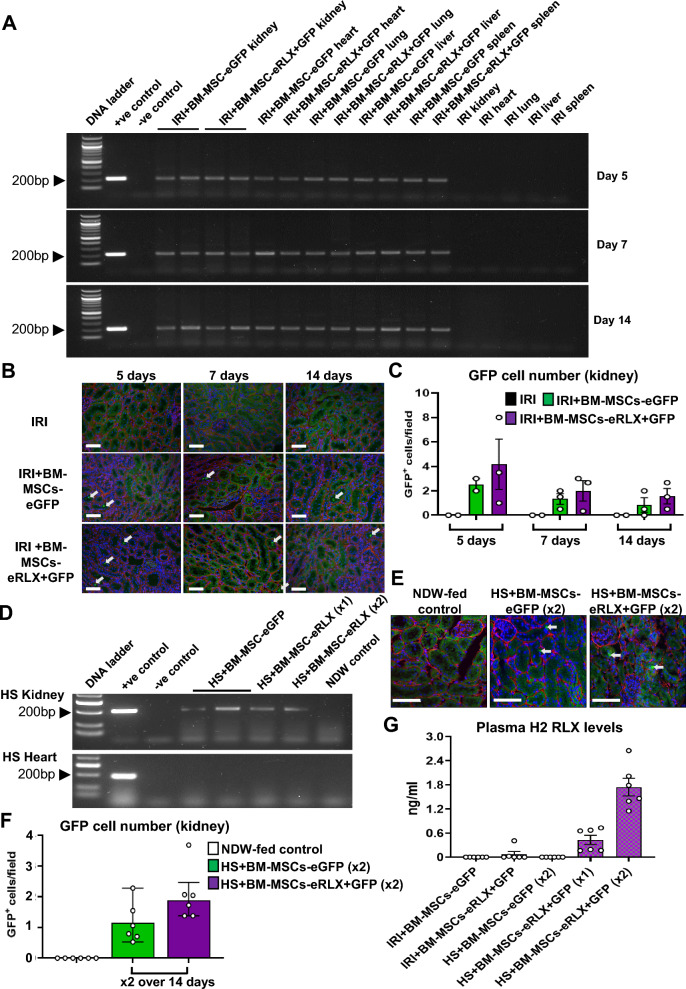
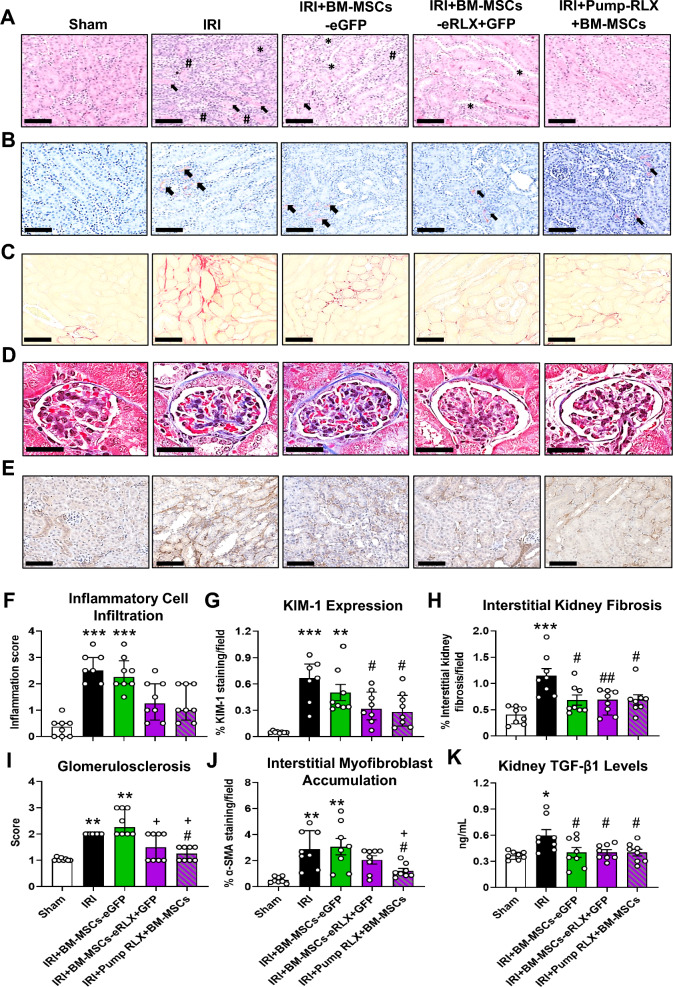
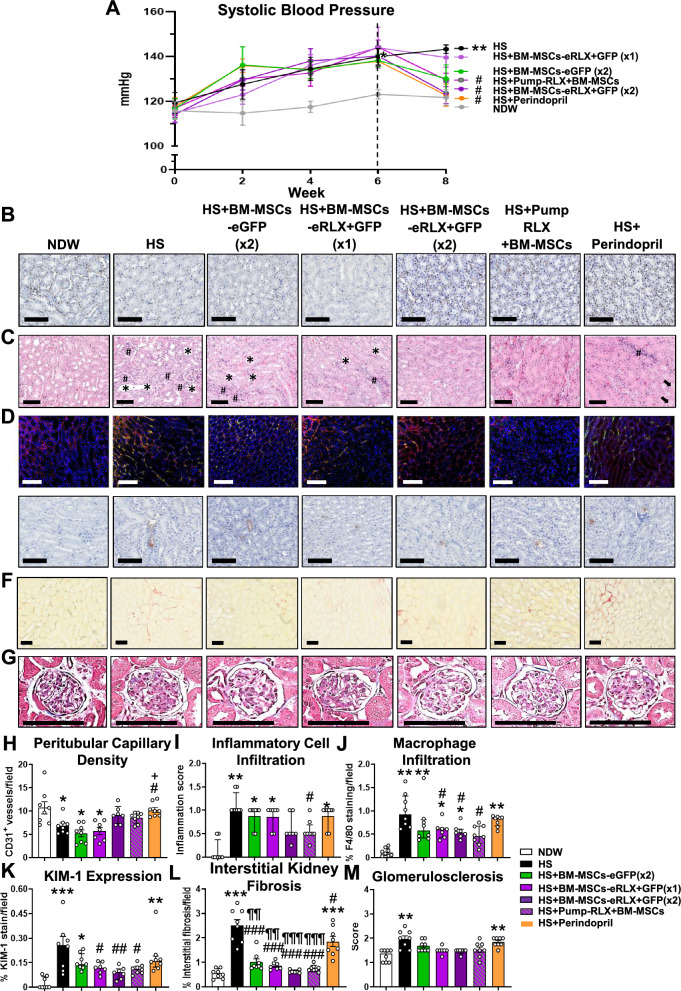
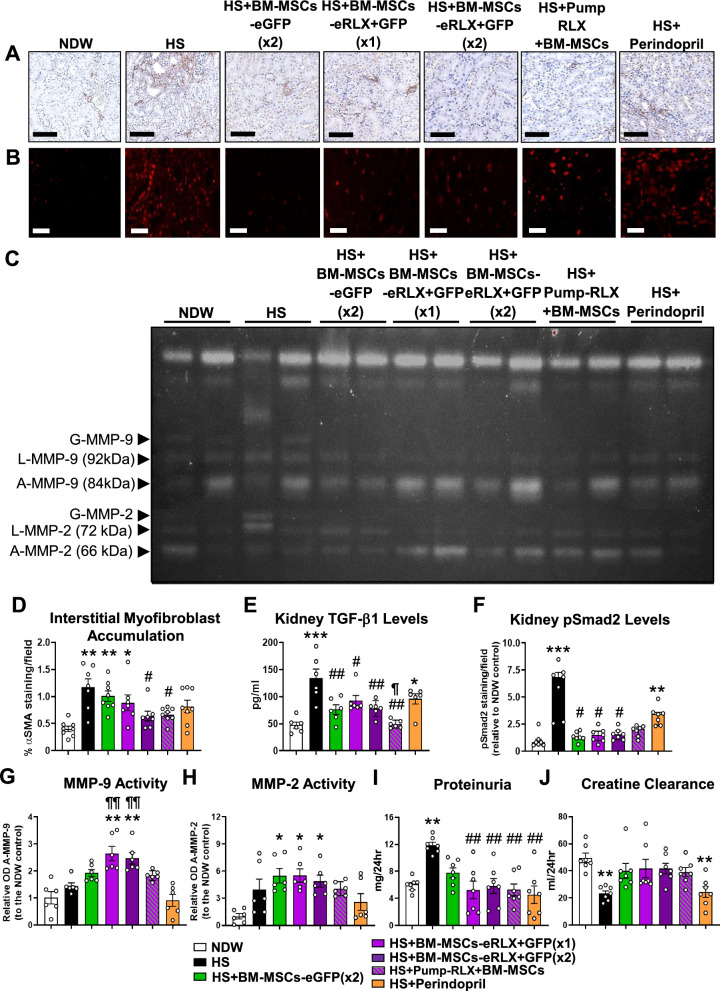
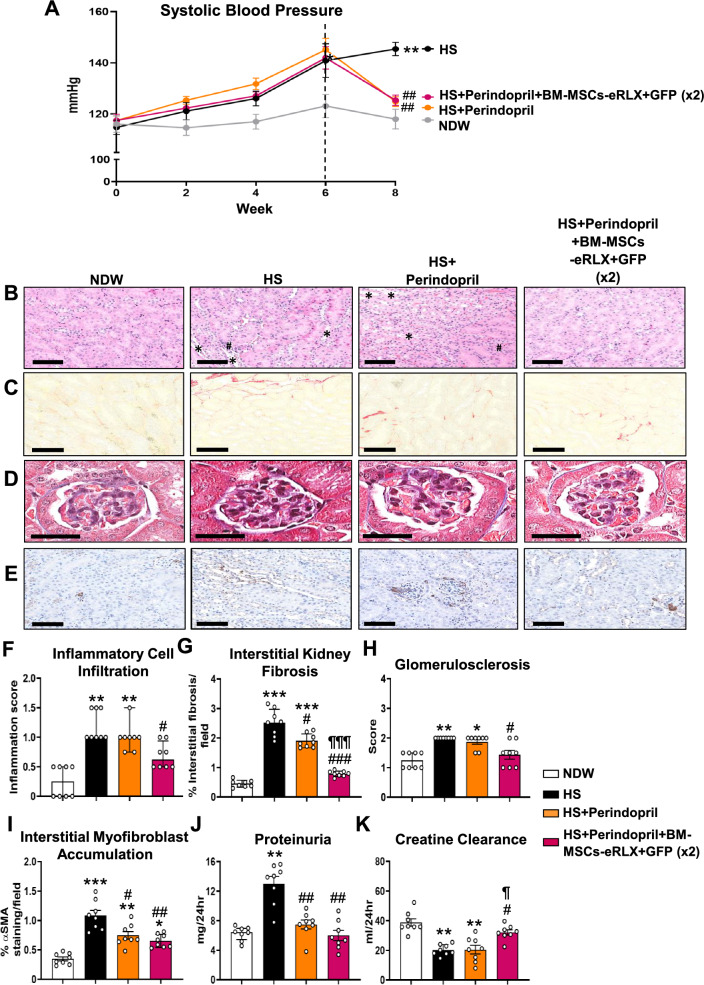
When cultured for 3- or 7-days in vitro, 1 × 10 BM-MSCs-eRLX + GFP produced therapeutic RLX levels, and secreted an enhanced but finely-tuned cytokine profile without compromising their proliferation or differentiation capacity compared to naïve BM-MSCs. BM-MSCs-eRLX + GFP were identified in the kidney 2-weeks post-administration and retained the therapeutic effects of RLX in vivo. 1-2 × 10 BM-MSCs-eRLX + GFP attenuated the IRI- or therapeutically abrogated the HS-induced tubular epithelial damage and interstitial fibrosis, and significantly reduced the HS-induced hypertension, glomerulosclerosis and proteinuria. This was to an equivalent extent as RLX and BM-MSCs administered separately but to a broader extent than BM-MSCs-eGFP or the angiotensin-converting enzyme inhibitor, perindopril. Additionally, these renoprotective effects of BM-MSCs-eRLX + GFP were maintained in the presence of perindopril co-treatment, highlighting their suitability as adjunct therapies to ACE inhibition. Importantly, no major long-term adverse effects of BM-MSCs-eRLX + GFP were observed.
BM-MSCs-eRLX + GFP produced greater renoprotective and therapeutic efficacy over that of BM-MSCs-eGFP or ACE inhibition, and may represent a novel and safe treatment option for acute kidney injury and hypertensive CKD.
肾纤维化是慢性肾脏病(CKD)的标志,并损害了移植的人骨髓间充质基质细胞(BM-MSCs)的活力。因此,BM-MSCs 被遗传工程改造以表达抗纤维化和肾保护激素人松弛素-2(RLX)和绿色荧光蛋白(BM-MSCs-eRLX+GFP),这使得 BM-MSCs-eRLX+GFP 能够通过单次静脉注射进行传递。
BM-MSCs 通过慢病毒转导带有人类松弛素-2 cDNA 和 GFP,在真核翻译延伸因子-1α启动子(BM-MSCs-eRLX+GFP)或 GFP 单独(BM-MSCs-eGFP)下。评估了 BM-MSCs-eRLX+GFP 在体外分化、增殖、迁移、产生 RLX 和细胞因子的能力,而在缺血再灌注损伤(IRI)和高盐(HS)诱导的高血压 CKD 的临床前模型中评估了 BM-MSCs-eRLX+GFP 归巢至损伤肾脏和肾保护作用。还在体内治疗停止后 9 个月确定了 BM-MSCs-RLX+GFP 的长期安全性。
当在体外培养 3 或 7 天时,1×10 BM-MSCs-eRLX+GFP 产生了治疗性 RLX 水平,并分泌了增强但精细调节的细胞因子谱,而不会损害其增殖或分化能力与原始 BM-MSCs 相比。BM-MSCs-eRLX+GFP 在给药后 2 周被鉴定在肾脏中,并在体内保留了 RLX 的治疗作用。1-2×10 BM-MSCs-eRLX+GFP 减轻了 IRI 或治疗性阻断的 HS 诱导的肾小管上皮损伤和间质纤维化,并显著降低了 HS 诱导的高血压、肾小球硬化和蛋白尿。与单独给予 RLX 或 BM-MSCs 相比,其效果相当,但比 BM-MSCs-eGFP 或血管紧张素转换酶抑制剂培哚普利的效果更广泛。此外,在培哚普利联合治疗的情况下,BM-MSCs-eRLX+GFP 的这些肾保护作用得以维持,这突出了它们作为 ACE 抑制的辅助治疗的适用性。重要的是,没有观察到 BM-MSCs-eRLX+GFP 的主要长期不良影响。
与 BM-MSCs-eGFP 或 ACE 抑制相比,BM-MSCs-eRLX+GFP 产生了更大的肾保护和治疗效果,可能代表了急性肾损伤和高血压 CKD 的一种新的安全治疗选择。