Michael Arwed Elias, Schoenbeck Denise, Becker-Assmann Jendrik, Haag Nina Pauline, Niehoff Julius Henning, Schmidt Bernhard, Panknin Christoph, Baer-Beck Matthias, Hickethier Tilman, Maintz David, Bunck Alexander C, Gertz Roman Johannes, Borggrefe Jan, Kroeger Jan Robert
Department of Radiology, Neuroradiology and Nuclear Medicine, Johannes Wesling University Hospital, Ruhr University Bochum, 44801 Bochum, Germany.
Siemens Healthineers AG, 91301 Forchheim, Germany.
BJR Open. 2024 Oct 18;6(1):tzae030. doi: 10.1093/bjro/tzae030. eCollection 2024 Jan.
Coronary CT angiography (CCTA) is becoming increasingly important in the workup of coronary artery disease. Imaging of stents and in-stent stenoses remains a challenge. This work investigates the assessability of in-stent stenoses in photon counting CT (PCCT) using ultra-high-resolution (UHR) imaging and optimized reconstruction kernels.
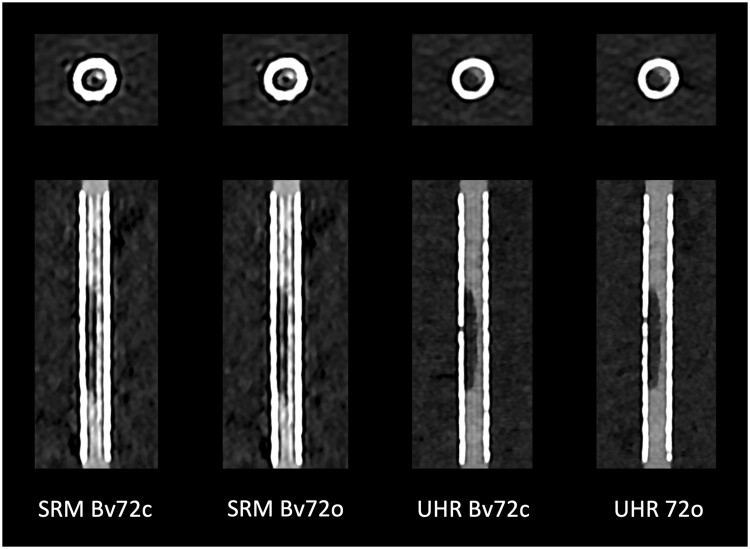
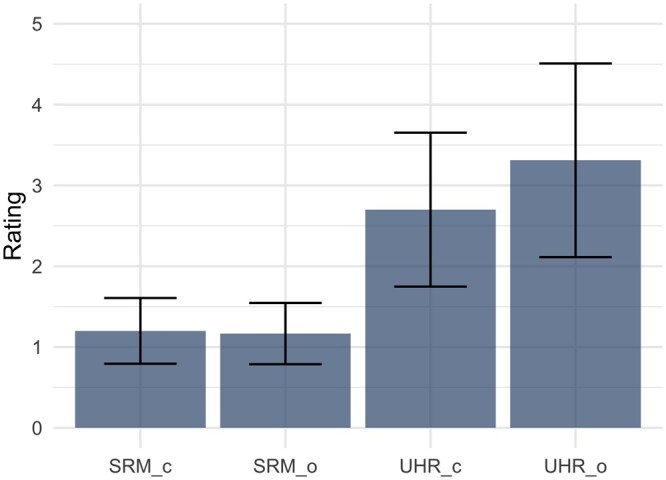
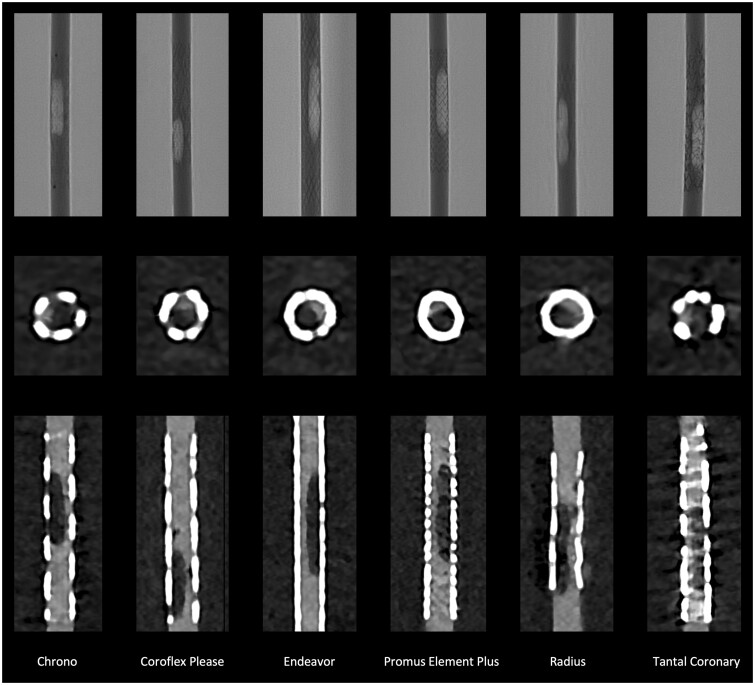
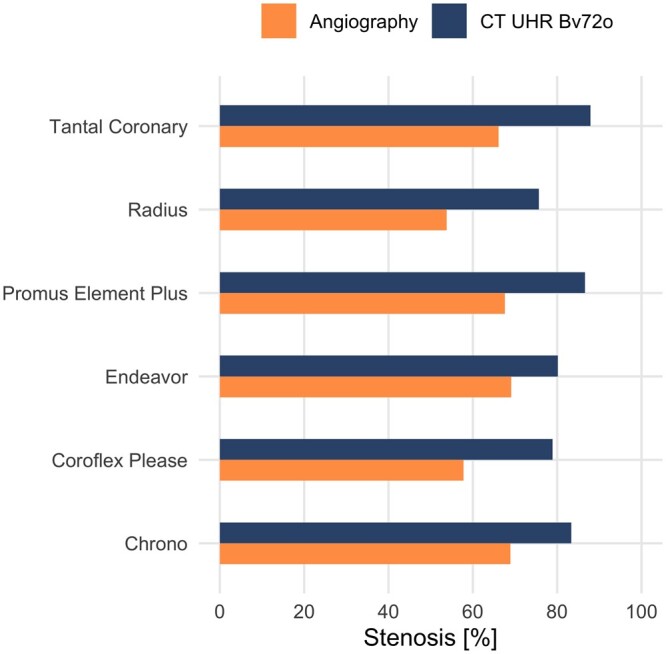
In an established phantom, 6 stents with inserted hypodense stenoses were scanned in both standard resolution (SRM) and UHR in a clinical PCCT scanner (NAEOTOM Alpha, Siemens Healthineers, Germany). Reconstructions were made both with the clinically established and optimized kernels. The visible stent lumen and the extent of stenosis were quantitatively measured and compared with the angiographic reference standard. Also, region-of-interest (ROI)-based measurements and a qualitative assessment of image quality were performed.
The visible stent lumen and the extent of stenosis were measured more precisely in UHR compared to SRM (0.11 ± 0.19 vs 0.41 ± 0.22 mm, < .001). The optimized kernel further improved the accuracy of the measurements and image quality in UHR (0.35 ± 0.23 vs 0.47 ± 0.19 mm, < .001). Compared to angiography, stenoses were overestimated in PCCT, on average with an absolute difference of 18.20% ± 4.11%.
Photon counting CCTA allows improved imaging of in-stent stenoses in a phantom using UHR imaging and optimized kernels. These results support the use of UHR and optimized kernels in clinical practice and further studies.
UHR imaging and optimized reconstruction kernels should be used in CCTA in the presence of cardiac stents.
冠状动脉CT血管造影(CCTA)在冠状动脉疾病的检查中变得越来越重要。支架及支架内狭窄的成像仍然是一项挑战。本研究使用超高分辨率(UHR)成像和优化的重建内核,探讨光子计数CT(PCCT)对支架内狭窄的可评估性。
在一个已建立的模型中,对6个插入低密度狭窄的支架在临床PCCT扫描仪(德国西门子医疗的NAEOTOM Alpha)上进行标准分辨率(SRM)和UHR扫描。使用临床既定的和优化的内核进行重建。定量测量可见的支架管腔和狭窄程度,并与血管造影参考标准进行比较。此外,还进行了基于感兴趣区域(ROI)的测量和图像质量的定性评估。
与SRM相比,UHR能更精确地测量可见的支架管腔和狭窄程度(0.11±0.19 vs 0.41±0.22 mm,P<0.001)。优化内核进一步提高了UHR测量的准确性和图像质量(0.35±0.23 vs 0.47±0.19 mm,P<0.001)。与血管造影相比,PCCT对狭窄的估计过高,平均绝对差异为18.20%±4.11%。
光子计数CCTA使用UHR成像和优化内核,能够改善模型中支架内狭窄的成像。这些结果支持在临床实践和进一步研究中使用UHR和优化内核。
在存在心脏支架的情况下,CCTA应使用UHR成像和优化的重建内核。