Aternali Andrea, Lumsden-Ruegg Heather, Appel Lora, Hitzig Sander L, Mayo Amanda L, Katz Joel
Department of Psychology, York University, Toronto, ON, Canada.
School of Health Policy & Management, York University, Toronto, ON, Canada.
Front Pain Res (Lausanne). 2024 Oct 9;5:1409352. doi: 10.3389/fpain.2024.1409352. eCollection 2024.
Individuals with limb loss frequently report post-amputation phenomena, including nonpainful phantom sensations, phantom limb pain (PLP), and residual limb pain (RLP). Although post-amputation pain is common, not all patients benefit from widely accepted treatments. A greater understanding of phantom limb "telescoping", the experience of one's phantom hand or foot gradually approaching the residual limb, may assist in developing more effective interventions for reducing post-amputation pain. This case report explores the relationships between PLP, RLP, telescoping, and psychosocial experience in one person with a lower limb amputation. The aim of this case is to illustrate one possible relationship between telescoping and PLP as the mechanisms linking the two remain equivocal.
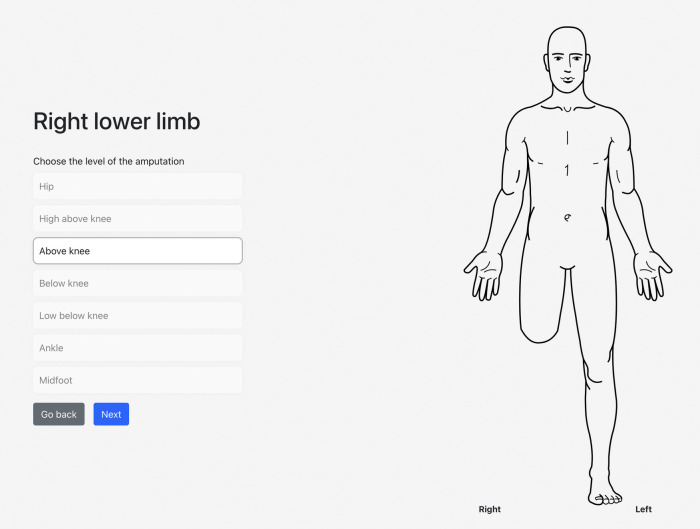
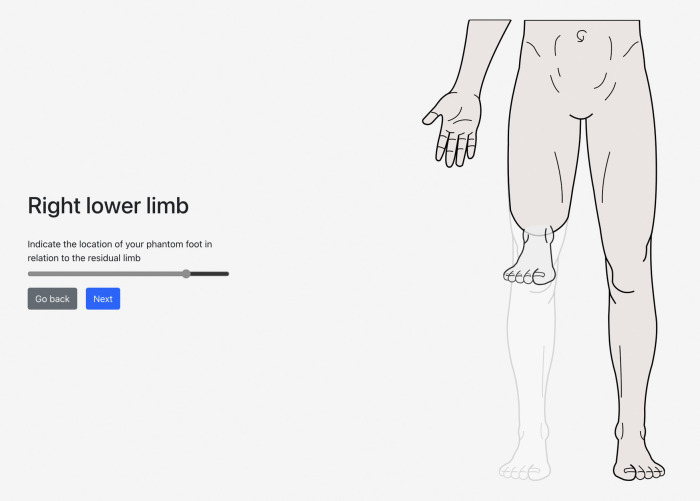
The participant is a 35-year-old male who underwent a transfemoral amputation due to a traumatic injury to his right leg approximately 4 years prior. He responded to questionnaires evaluating demographic and health-related information (e.g., age, sex, marital status, reason for amputation), pain and psychological variables via the Brief Pain Inventory (BPI-SF), ID Pain Questionnaire (IDPQ), Pain Catastrophizing Scale (PSC-4), Patient Health Questionnaire-4 (PHQ-4), Life Orientation Test-Revised (LOT-R), Connor-Davidson Resilience Scale (CD-RISC2), and Chronic Pain Acceptance Questionnaire (CPAQ-8) and telescoping, measured by a newly developed app. The participant completed a semi-structured interview that was designed to ascertain patterns in the overlapping experience of phantom limb telescoping and post-amputation pain.
The participant rated his average PLP as 10 on a Numeric Rating Scale (NRS) from 0 ("no pain") to 10 ("worst pain imaginable") shortly after amputation. Approximately 12 months later, the participant noticed a shortening of his phantom limb, with a concurrent decrease in PLP. At present, his average NRS pain intensity is a 5/10. The participant described how the daily, debilitating PLP intensity diminished to weekly, manageable pain over time. Most notably, his responses on questionnaires were consistent with neuropathic PLP, mild to moderate levels of pain interference, a high level of catastrophic thinking about pain, low optimism, and mild symptoms of anxiety and depression.
In this report, telescoping appeared to be preceded by an initial reduction in PLP intensity but these findings are based on a single case report and must be replicated with a large sample size before we have a clearer idea of the relationship between telescoping and PLP. This study provides insight into factors that may maintain PLP, generating targets for further investigation.
肢体缺失者经常报告截肢后出现的现象,包括无痛性幻肢感觉、幻肢痛(PLP)和残肢痛(RLP)。尽管截肢后疼痛很常见,但并非所有患者都能从广泛接受的治疗中获益。对幻肢“套叠”(即幻手或幻足逐渐靠近残肢的体验)有更深入的了解,可能有助于开发更有效的干预措施来减轻截肢后疼痛。本病例报告探讨了一名下肢截肢患者的幻肢痛、残肢痛、套叠现象与心理社会体验之间的关系。本病例的目的是阐明套叠现象与幻肢痛之间一种可能的关系,因为两者之间的联系机制尚不明确。
参与者是一名35岁男性,约4年前因右腿外伤接受了经股骨截肢手术。他通过填写问卷来评估人口统计学和健康相关信息(如年龄、性别、婚姻状况、截肢原因),通过简短疼痛问卷(BPI-SF)、ID疼痛问卷(IDPQ)、疼痛灾难化量表(PSC-4)、患者健康问卷-4(PHQ-4)、生活取向测试修订版(LOT-R)、康纳-戴维森复原力量表(CD-RISC2)和慢性疼痛接受问卷(CPAQ-8)评估疼痛和心理变量,并用一个新开发的应用程序测量套叠现象。参与者完成了一次半结构化访谈,旨在确定幻肢套叠和截肢后疼痛重叠体验中的模式。
截肢后不久,参与者在数字评分量表(NRS,范围从0分“无疼痛”到10分“想象中的最剧烈疼痛”)上对其平均幻肢痛评分为10分。大约12个月后,参与者注意到他的幻肢缩短,同时幻肢痛有所减轻。目前,他的平均NRS疼痛强度为5/10。参与者描述了随着时间推移,日常使人衰弱的幻肢痛强度如何逐渐减轻为每周可控制的疼痛。最值得注意的是,他在问卷上的回答与神经性幻肢痛、轻度至中度的疼痛干扰、对疼痛的高度灾难化思维、低乐观度以及焦虑和抑郁的轻度症状相符。
在本报告中,套叠现象似乎在幻肢痛强度最初降低之后出现,但这些发现基于单个病例报告,在我们更清楚地了解套叠现象与幻肢痛之间的关系之前,必须用大样本进行重复验证。本研究为可能维持幻肢痛的因素提供了见解,为进一步研究提供了目标。