Lee June, Kim Yong Han, Lim Hyun Ah, Hong Seok Beom, Kim Do Yeon, Kim Hwan Wook
Department of Thoracic and Cardiovascular Surgery, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Republic of Korea.
J Thorac Dis. 2024 Sep 30;16(9):6171-6181. doi: 10.21037/jtd-23-1942. Epub 2024 May 7.
Biological valve prostheses in rapid-deployment aortic valve replacement (RD AVR) procedures have demonstrated excellent outcomes. However, previous studies indicate a lack of specific surgical outcomes for the bicuspid aortic valve (BAV) or recommend RD AVR implementation. The existing literature comparing the clinical and hemodynamic outcomes of patients with BAV and those with tricuspid aortic valves (TAVs) after RD AVR is limited. Therefore, this study evaluated the safety and feasibility of RD AVR in BAV, including Sievers type 0, and compared the early clinical and hemodynamic outcomes of patients who underwent RD AVR at a single center based on aortic valve type.
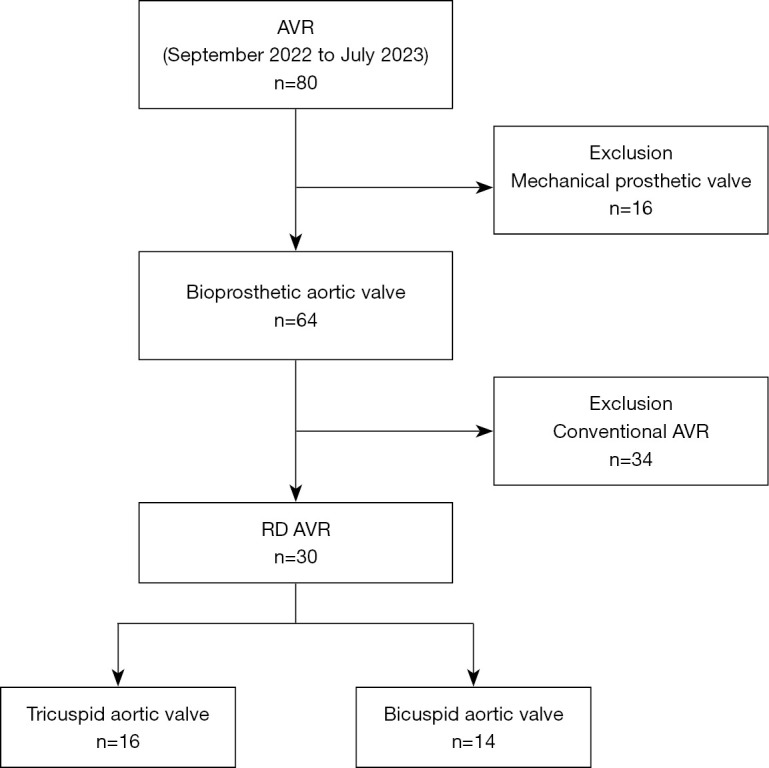
Our institution officially commenced performing RD AVR using Intuity valves in September 2022. The medical records of 80 patients who underwent aortic valve replacement (AVR) between September 1, 2022, and July 31, 2023 were retrospectively analyzed. In this set, 30 patients underwent RD AVR for aortic stenosis. Among the 30 RD AVR cases, groups A and B comprised 16 (53.3%) patients with TAV and 14 (46.7%) with BAV, respectively. The preoperative characteristics and postoperative echocardiographic data were compared between the two groups.
No statistically significant differences in preoperative characteristics, including mean age and sex distribution, were found between groups A and B. Notably, no patient in both groups exhibited mild- or higher-grade aortic regurgitation. The postoperative transvalvular mean pressure gradients showed significantly lower values in group B than in group A (12.20±4.64 16.26±5.49 mmHg, P=0.03). The necessity to insert a permanent pacemaker was not found in any of the patients (0%) in group A but was found in one (7.1%) patient in group B (P=0.46). Among the BAV cases, six (20%) were categorized as Sievers type 0. Of the 14 patients in group B, six with Sievers type 0 and the remaining eight with other bicuspid valve types were designated as groups B0 and B1, respectively. Similarly, no significant difference in postoperative transvalvular mean pressure gradient was observed between the two groups (11.33±4.49 12.86±4.94 mmHg, P=0.56). No in-hospital mortality was observed among all 30 patients.
In this study, RD AVR was considered feasible in a small, carefully selected cohort of patients with aortic stenosis, even in BAV, including Sievers type 0, as observed from the standpoint of postoperative hemodynamic outcomes and the incidence of aortic regurgitation.
快速部署主动脉瓣置换术(RD AVR)中使用的生物瓣膜假体已显示出优异的效果。然而,先前的研究表明,对于二叶式主动脉瓣(BAV)缺乏具体的手术结果,或者建议实施RD AVR。现有文献比较RD AVR后BAV患者与三尖瓣主动脉瓣(TAV)患者的临床和血流动力学结果有限。因此,本研究评估了RD AVR在BAV(包括Sievers 0型)中的安全性和可行性,并根据主动脉瓣类型比较了在单一中心接受RD AVR的患者的早期临床和血流动力学结果。
我们机构于2022年9月正式开始使用Intuity瓣膜进行RD AVR。回顾性分析了2022年9月1日至2023年7月31日期间80例行主动脉瓣置换术(AVR)患者的病历。在这一组中,30例患者因主动脉瓣狭窄接受RD AVR。在30例RD AVR病例中,A组和B组分别包括16例(53.3%)TAV患者和14例(46.7%)BAV患者。比较两组患者的术前特征和术后超声心动图数据。
A组和B组在术前特征(包括平均年龄和性别分布)方面未发现统计学上的显著差异。值得注意的是,两组均无患者出现轻度或更高级别的主动脉瓣反流。术后跨瓣平均压力梯度显示,B组显著低于A组(12.20±4.64对16.26±5.49 mmHg,P=0.03)。A组患者均未发现有必要植入永久性起搏器(0%),而B组有1例(7.1%)患者需要植入(P=0.46)。在BAV病例中,6例(20%)被归类为Sievers 0型。在B组的14例患者中,6例Sievers 0型和其余8例其他二叶式瓣膜类型分别被指定为B0组和B1组。同样,两组术后跨瓣平均压力梯度无显著差异(11.33±4.49对12.86±4.94 mmHg,P=0.56)。30例患者均未观察到院内死亡。
在本研究中,从术后血流动力学结果和主动脉瓣反流发生率来看,即使是在包括Sievers 0型的BAV患者中,RD AVR在一小群经过精心挑选的主动脉瓣狭窄患者中被认为是可行的。