Brown Bailey, Le Tan, Naeem Aroma, Malik Aroosa, Norton Elizabeth L, Wu Xiaoting, Patel Himanshu J, Deeb G Michael, Kim Karen M, Yang Bo
Department of Cardiac Surgery, Michigan Medicine, Ann Arbor, Mich.
Creighton University School of Medicine, Omaha, Neb.
JTCVS Open. 2021 Sep 28;8:177-188. doi: 10.1016/j.xjon.2021.09.033. eCollection 2021 Dec.
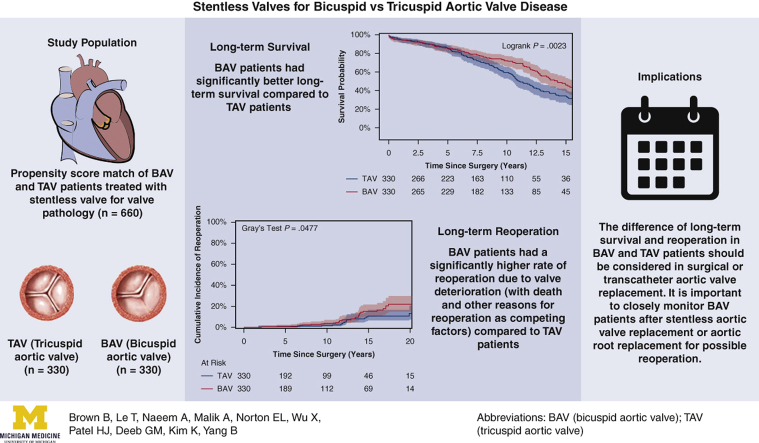
To determine long-term survival and reoperation rate in patients with a bicuspid aortic valve (BAV) and patients with a tricuspid aortic valve (TAV) after stentless aortic valve replacement (AVR)/aortic root replacement (ARR).
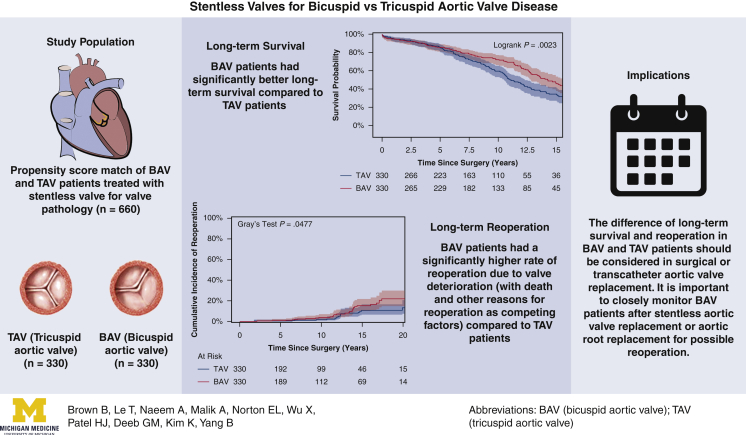
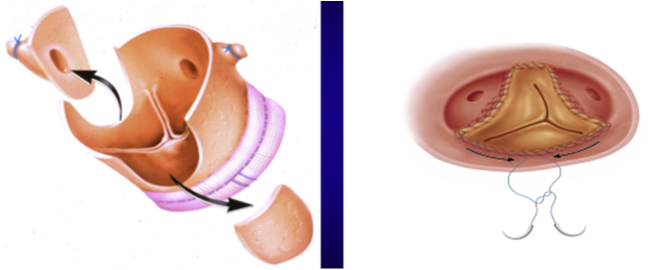
Between 1992 and 2014, 1293 patients underwent first AVR/ARR with a stentless aortic valve using the modified inclusion operating technique, including 741 patients with a TAV and 552 with a BAV. Using propensity scoring with 26 variables, 330 matched pairs were identified with AVR with or without ascending aorta/arch replacement. Data were obtained through chart review, surveys, and the National Death Index.
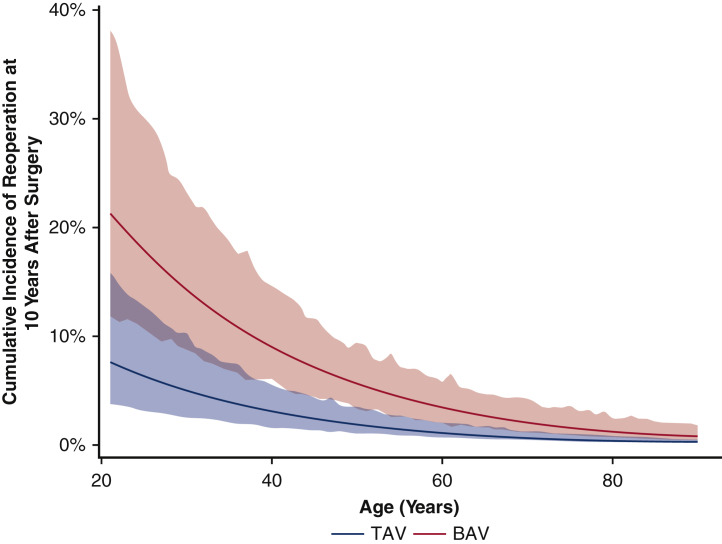
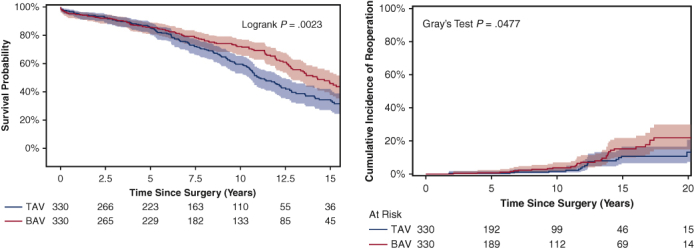
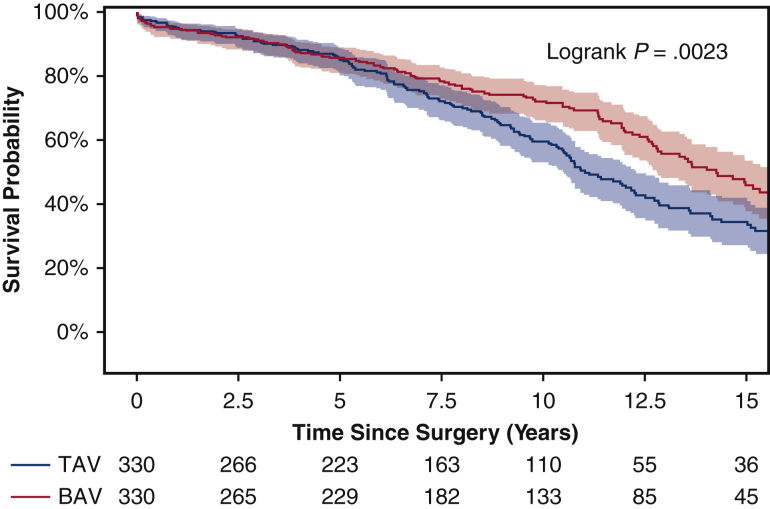
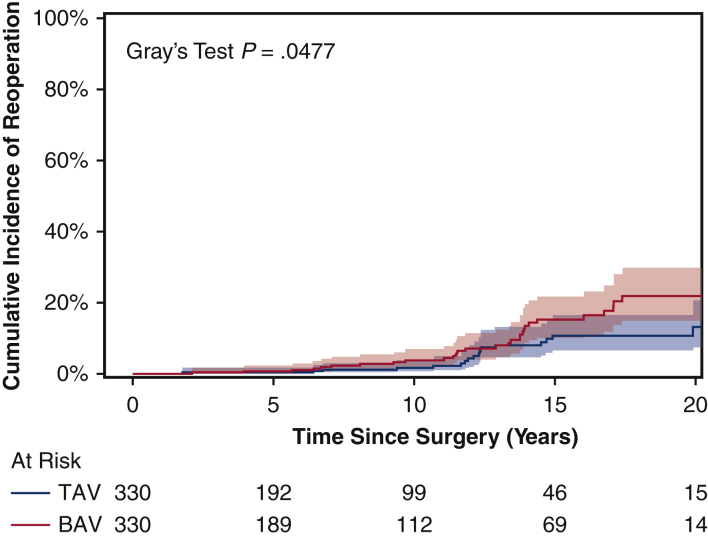
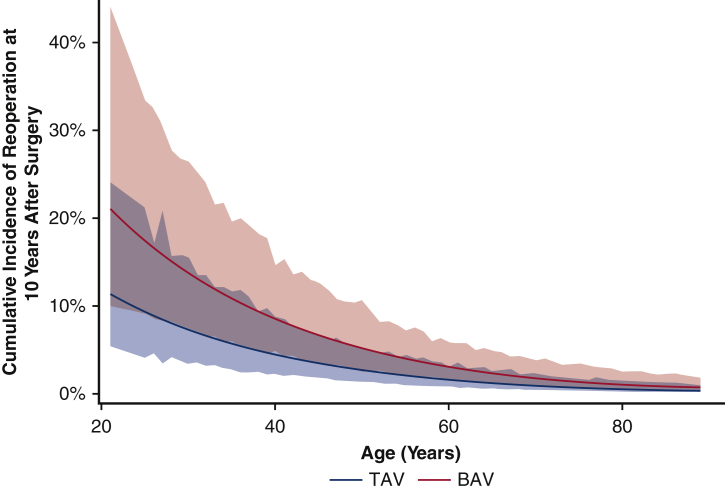
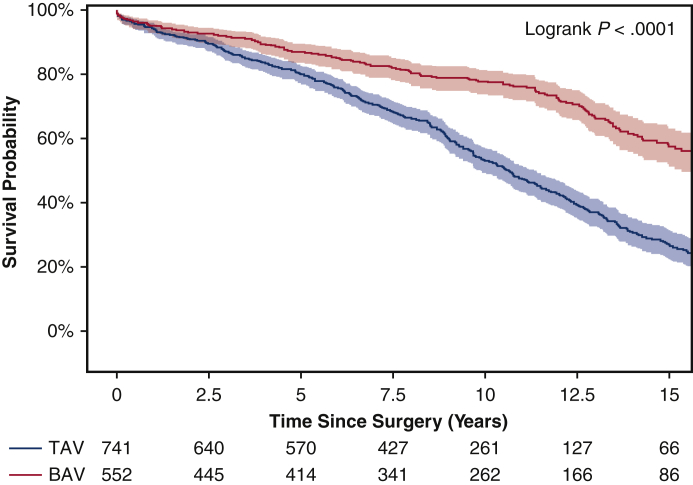
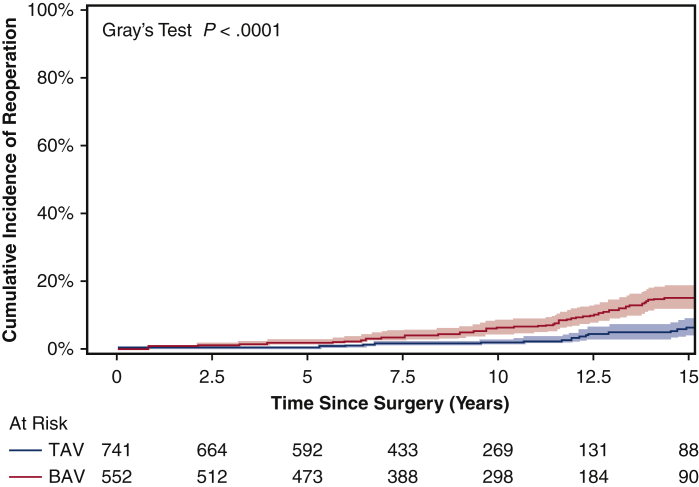
Patient demographics were similar in the propensity score-matched groups. Both groups had similar cardiopulmonary bypass, cross-clamp, and hypothermia circulatory arrest times, cerebral protection strategies, and rate of aortic arch replacement. The median size of implanted valves was similar (BAV: 27 mm [range, 25-29 mm] vs TAV: 27 mm [range, 25-27 mm]). Compared with the TAV group, the BAV group had a shorter hospital stay (6 days vs 7 days; = .001) but similar 30-day mortality (1.8% vs 1.2%). The BAV group had better long-term (15-year) survival (46% vs 33%; = .002) but a higher cumulative incidence of reoperation for structural valve deterioration (15-year: 15% vs 11%; = .048). Cox proportional hazard analysis identified a BAV as a protective factor for long-term mortality (hazard ratio [HR], 0.71; 95% CI, 0.56-0.91; = .006), but a risk factor for reoperation due to structural valve deterioration (HR, 1.4 [95% CI, 0.8-2.6; = .27] in the matched cohort and 2.2 [95% CI, 1.3-3.7; = .004] in the unmatched cohort).
The BAV patients had better long-term survival but a higher reoperation rate compared with TAV patients after stentless AVR. Our findings suggest caution in the use of bioprostheses for BAV patients.
确定在无支架主动脉瓣置换术(AVR)/主动脉根部置换术(ARR)后,二叶式主动脉瓣(BAV)患者和三叶式主动脉瓣(TAV)患者的长期生存率及再次手术率。
1992年至2014年期间,1293例患者采用改良的纳入手术技术接受了首次使用无支架主动脉瓣的AVR/ARR,其中包括741例TAV患者和552例BAV患者。通过对26个变量进行倾向评分,确定了330对匹配的接受或未接受升主动脉/主动脉弓置换的AVR患者。数据通过病历审查、调查和国家死亡指数获得。
倾向评分匹配组的患者人口统计学特征相似。两组的体外循环、主动脉阻断和低温循环停搏时间、脑保护策略以及主动脉弓置换率相似。植入瓣膜的中位尺寸相似(BAV:27mm[范围25 - 29mm] vs TAV:27mm[范围25 - 27mm])。与TAV组相比,BAV组住院时间较短(6天vs 7天;P = 0.001),但30天死亡率相似(1.8% vs 1.2%)。BAV组长期(15年)生存率更高(46% vs 33%;P = 0.002),但因结构性瓣膜退变导致的再次手术累积发生率更高(15年:15% vs 11%;P = 0.048)。Cox比例风险分析确定BAV是长期死亡率的保护因素(风险比[HR],0.71;95%可信区间[CI],0.56 - 0.91;P = 0.006),但却是因结构性瓣膜退变导致再次手术的风险因素(在匹配队列中HR为1.4[95%CI,0.8 - 2.6;P = 0.27],在未匹配队列中HR为2.2[95%CI,1.3 - 3.7;P = 0.004])。
与无支架AVR术后的TAV患者相比,BAV患者长期生存率更高,但再次手术率更高。我们的研究结果提示在BAV患者中使用生物假体时应谨慎。