Department of Surgery, Hepato-Pancreato-Biliary and Digestive Surgery Unit, Faculty of Medicine, Alexandria University, Alexandria, Egypt.
BMC Surg. 2024 Oct 24;24(1):329. doi: 10.1186/s12893-024-02532-x.
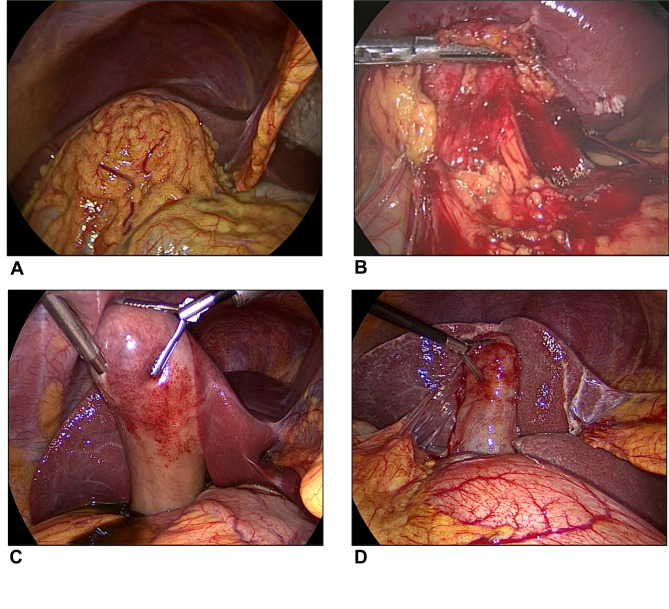
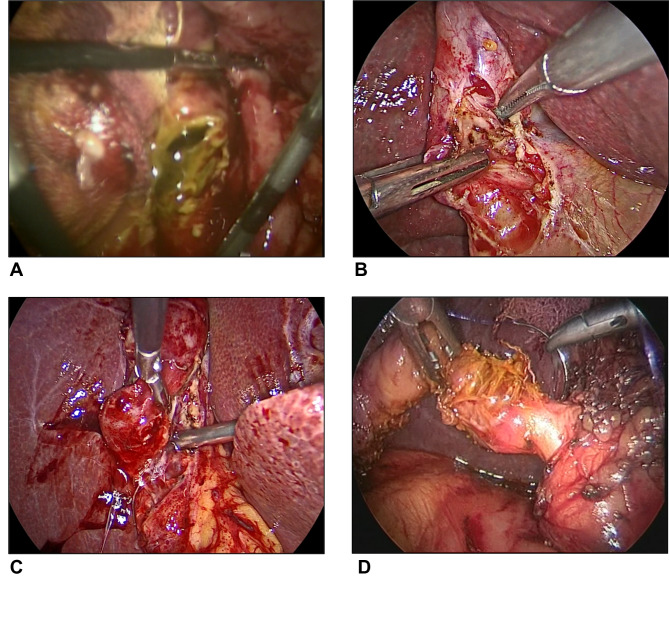
Early laparoscopic cholecystectomy (ELC) in the setting of acute calculous cholecystitis (ACC) requires to be performed by highly-skilled surgeons to avoid complications. The purpose of this study is to identify preoperative factors that would predict difficult ELC among patients with ACC prior to proceeding with surgery.
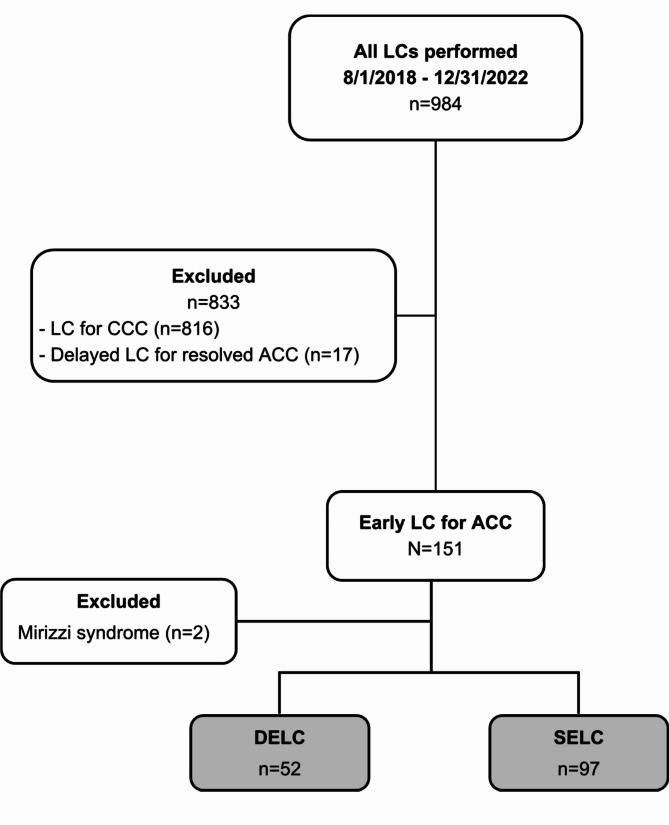
We retrospectively reviewed all patients who received ELC within 10 days from the onset of symptoms of ACC between August 1, 2018, and December 31, 2022. They were divided into 2 groups according to the difficulty of surgery.
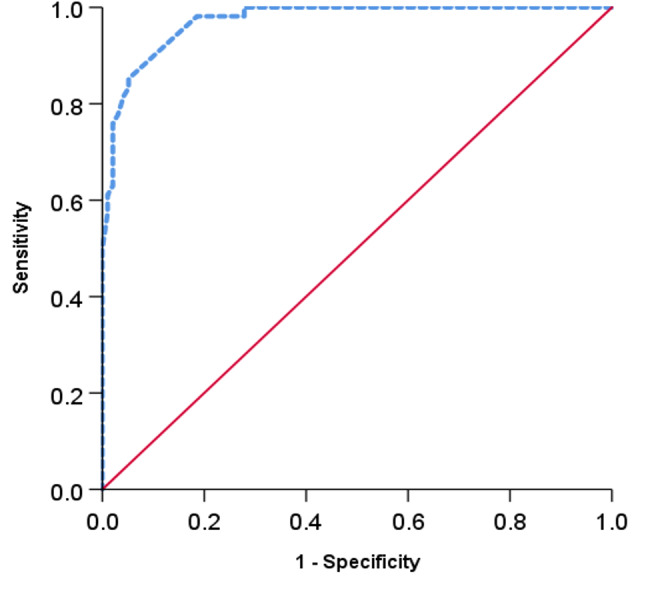
149 patients with ACC received ELC during the study period. ELC was considered difficult in 52 patients (35%). Five preoperative factors were identified as significant predictors of difficult ELC (DELC) on multivariate analysis: duration of acute attack ≥ 4 days from the onset of symptoms till surgery (OR 34.4, P < 0.001), ultrasound showing largest gallstone size > 20 mm (OR 20.2, P = 0.029), ultrasound showing gallstone impaction in Hartmann's pouch (OR 7.2, P = 0.017), history of prior episode(s) of acute attack (OR 6.8, P = 0.048), and diabetes mellitus (OR 5.8, P = 0.046).
Careful preoperative assessment of patients with ACC is crucial among junior surgeons with limited surgical expertise prior to proceeding with ELC to identify those at risk of DELC to potentially reduce postoperative morbidity and mortality. If encountered, a management plan should be made, and surgery should proceed only upon confirming the availability of experienced surgeons in the field of biliary and laparoscopic surgery to supervise or assist in the procedure. Alternatively, such group of patients should rather be transferred to more advanced surgical centers which offer higher level of care to maintain patient safety and optimal surgical outcomes. More importantly, bail-out procedures should always be resorted to whenever DELC is encountered intraoperatively to prevent further surgical damage.
急性结石性胆囊炎(ACC)患者行早期腹腔镜胆囊切除术(ELC)需要由技术精湛的外科医生进行,以避免并发症。本研究旨在确定 ACC 患者在手术前可预测 ELC 难度的术前因素。
我们回顾性分析了 2018 年 8 月 1 日至 2022 年 12 月 31 日期间,ACC 症状发作后 10 天内接受 ELC 的所有患者。根据手术难度将其分为两组。
研究期间共有 149 例 ACC 患者接受了 ELC。52 例(35%)患者的 ELC 被认为困难。多因素分析显示,5 项术前因素是 DELC 的显著预测因素:急性发作持续时间≥症状发作至手术的 4 天(OR 34.4,P<0.001)、超声显示最大胆囊结石直径>20mm(OR 20.2,P=0.029)、超声显示胆囊结石嵌顿在Hartmann 袋(OR 7.2,P=0.017)、既往有急性发作史(OR 6.8,P=0.048)和糖尿病(OR 5.8,P=0.046)。
对于手术经验有限的初级外科医生,在进行 ELC 之前,对 ACC 患者进行仔细的术前评估至关重要,以识别出有 DELC 风险的患者,从而有可能降低术后发病率和死亡率。如果遇到这种情况,应制定管理计划,只有在确认有胆道和腹腔镜手术领域的经验丰富的外科医生在场监督或协助手术时,才能进行手术。或者,应将这类患者转至提供更高水平护理的更先进的外科中心,以确保患者安全和获得最佳手术效果。更重要的是,无论何时在术中遇到 DELC,都应采取紧急措施,以防止进一步的手术损伤。