Department of Clinical and Experimental Medicine, University of Pisa, Pisa, Italy.
Department of Clinical and Molecular Medicine, "La Sapienza" University, Via di Grottarossa, Rome, 1035-1039 - 00189, Italy.
Cardiovasc Diabetol. 2024 Oct 24;23(1):377. doi: 10.1186/s12933-024-02450-5.
A Chronic Kidney Disease (CKD) Epidemiology Collaboration (EPI) formula not including a Black race coefficient has been recently developed and is now recommended in the US. The new (2021) equation was shown to yield higher estimated glomerular filtration rate (eGFR) values than the old (2009) one in a non-Black general population sample, thus reclassifying a significant number of individuals to a better eGFR category. However, reclassified individuals were previously shown to have a lower risk of progression to end-stage kidney disease, but higher adjusted risks for all-cause death and morbidity and mortality from cardiovascular disease than those not reclassified. This study evaluated the prognostic impact of switching from the 2009 to the 2021 CKD-EPI equation in non-Black individuals with type 2 diabetes.
The Renal Insufficiency And Cardiovascular Events (RIACE) was a prospective cohort study enrolling 15,773 Caucasian patients in 19 Italian centers in 2006-2008. Cardiometabolic risk profile, treatments, complications, and comorbidities were assessed at baseline and eGFR was calculated with the two equations. Vital status was retrieved on 31 October 2015 for 15,656 participants (99.3%).
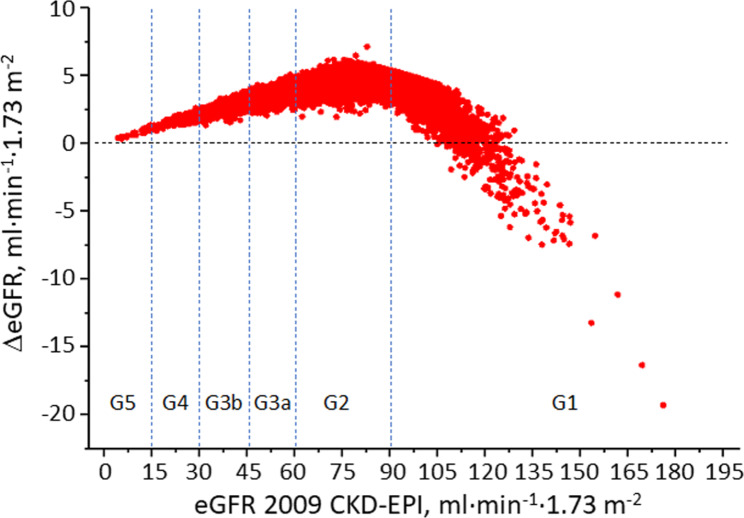
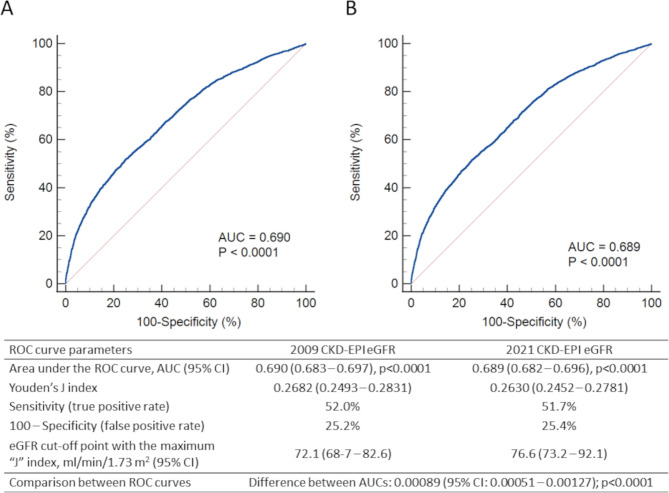
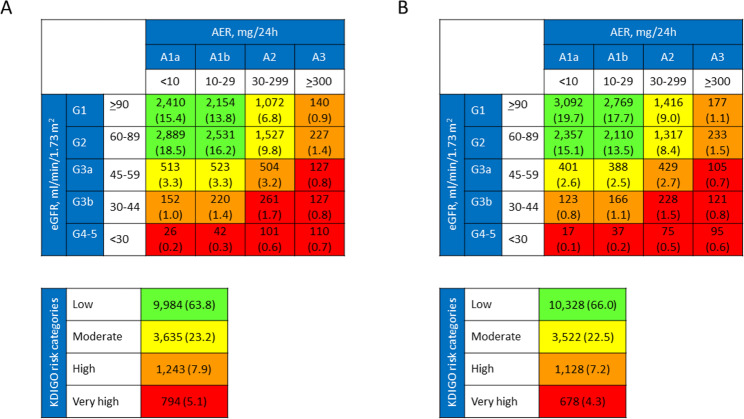
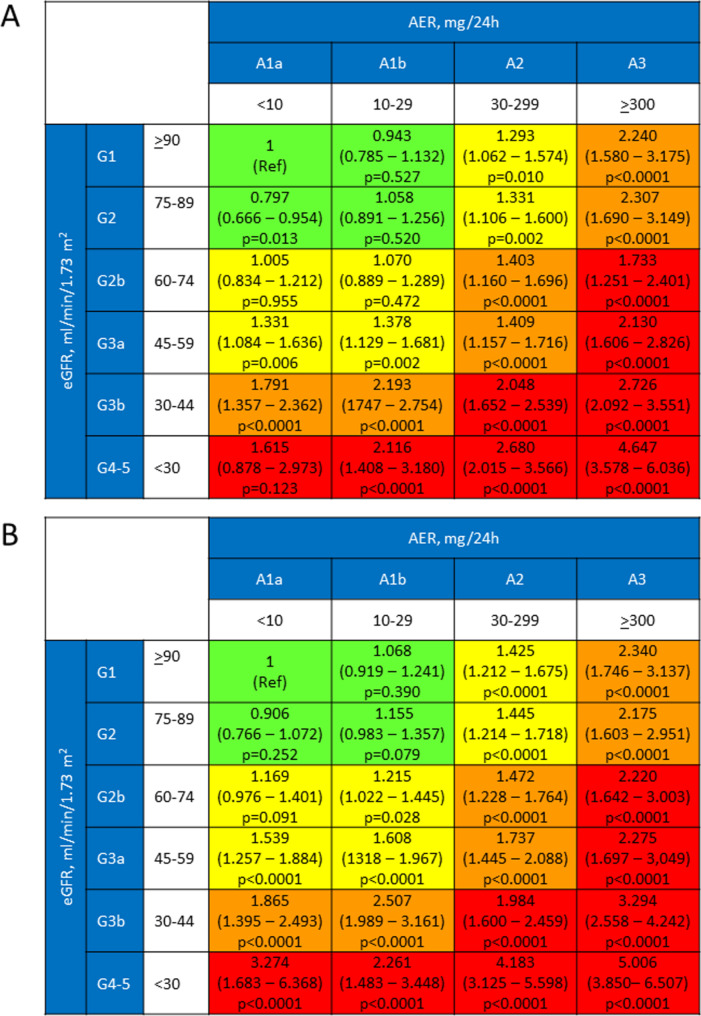
With the 2021 equation, the eGFR value increased in all patients, except for 293 individuals with a 2009 eGFR ≥ 105 ml·min·1.73 m. The median difference was 4.10 ml·min·1.73 m and was higher in males, older individuals and those in the G2 category. Reclassification decreased the percentage of patients with reduced eGFR from 17.28 to 13.96% and with any CKD from 36.23 to 34.03%. Reclassified individuals had better cardiometabolic risk profile and lower prevalence of complications and use of medications than non-reclassified individuals. Risk of death versus the 2009 G1 category was lower for reclassified than non-reclassified participants in all eGFR categories and, particularly, in each 2009 eGFR category, though difference was significant only in the G4-G5 category. The Receiver Operator Characteristic curves were statistically, but not clinically different with the two equations.
Changing from the 2009 to the 2021 CKD-EPI equation results in higher eGFR and lower CKD prevalence, with a lower risk of death in reclassified patients with an eGFR < 30 ml·min·1.73 m, but virtually no impact on mortality prediction.
ClinicalTrials.gov, NCT00715481, retrospectively registered 15 July, 2008.
最近开发了一种不包括黑人系数的慢性肾脏病(CKD)流行病学协作(EPI)公式,目前在美国推荐使用。在非黑人一般人群样本中,新的(2021 年)方程显示出比旧的(2009 年)方程更高的估计肾小球滤过率(eGFR)值,从而将大量个体重新分类到更好的 eGFR 类别。然而,之前已经表明,重新分类的个体进展为终末期肾病的风险较低,但全因死亡和心血管疾病的发病率和死亡率的调整风险较高。这项研究评估了在患有 2 型糖尿病的非黑人个体中,从 2009 年 CKD-EPI 方程转换为 2021 年 CKD-EPI 方程对预后的影响。
肾功能不全和心血管事件(RIACE)是一项前瞻性队列研究,于 2006 年至 2008 年在意大利 19 个中心招募了 15773 名白种人患者。在基线和 eGFR 时评估了心血管代谢风险状况、治疗方法、并发症和合并症,并使用两种方程进行计算。对于 15656 名参与者(99.3%),在 2015 年 10 月 31 日检索了生存状况。
在所有患者中,除了 293 名 2009 年 eGFR≥105ml·min·1.73·m 的患者外,2021 年 eGFR 值均升高。中位数差值为 4.10ml·min·1.73·m,男性、年龄较大的患者和 G2 类别的患者差值更高。重新分类使 eGFR 降低的患者比例从 17.28%降至 13.96%,任何 CKD 的患者比例从 36.23%降至 34.03%。与非重新分类患者相比,重新分类患者的心血管代谢风险状况更好,并发症和药物使用的发生率更低。与 2009 年 G1 类别相比,在所有 eGFR 类别中,重新分类患者的死亡率风险均低于非重新分类患者,尤其是在每个 2009 年 eGFR 类别中,但仅在 G4-G5 类别中差异具有统计学意义。两种方程的受试者工作特征曲线在统计学上有差异,但在临床上没有差异。
从 2009 年 CKD-EPI 方程改为 2021 年 CKD-EPI 方程会导致 eGFR 更高,CKD 患病率更低,eGFR<30ml·min·1.73·m 的重新分类患者死亡风险降低,但对死亡率预测几乎没有影响。
ClinicalTrials.gov,NCT00715481,2008 年 7 月 15 日回顾性注册。