Division of Orthopedic Surgery, Hillel Yaffe Medical Center, Ha-Shalom St,, 3820302, Hadera, Israel.
Faculty of Health Sciences, Joyce and Irving Goldman Medical School, Ben-Gurion University of the Negev, Beer-Sheva, Israel.
J Med Case Rep. 2024 Oct 30;18(1):527. doi: 10.1186/s13256-024-04865-w.
Spinal cord ischemic reperfusion injury is characterized by an abrupt decline in neurological function and only a few cases have been published in literature. Herein, we present a white cord syndrome following anterior decompression cervical fusion.
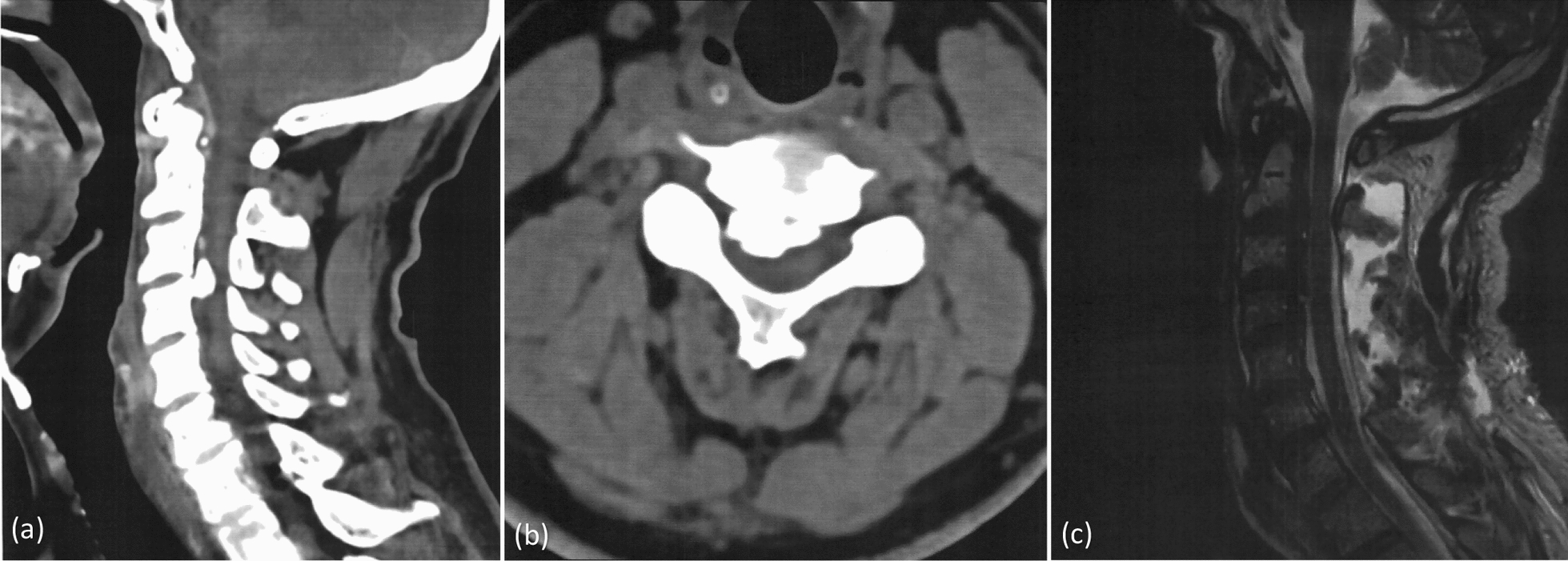
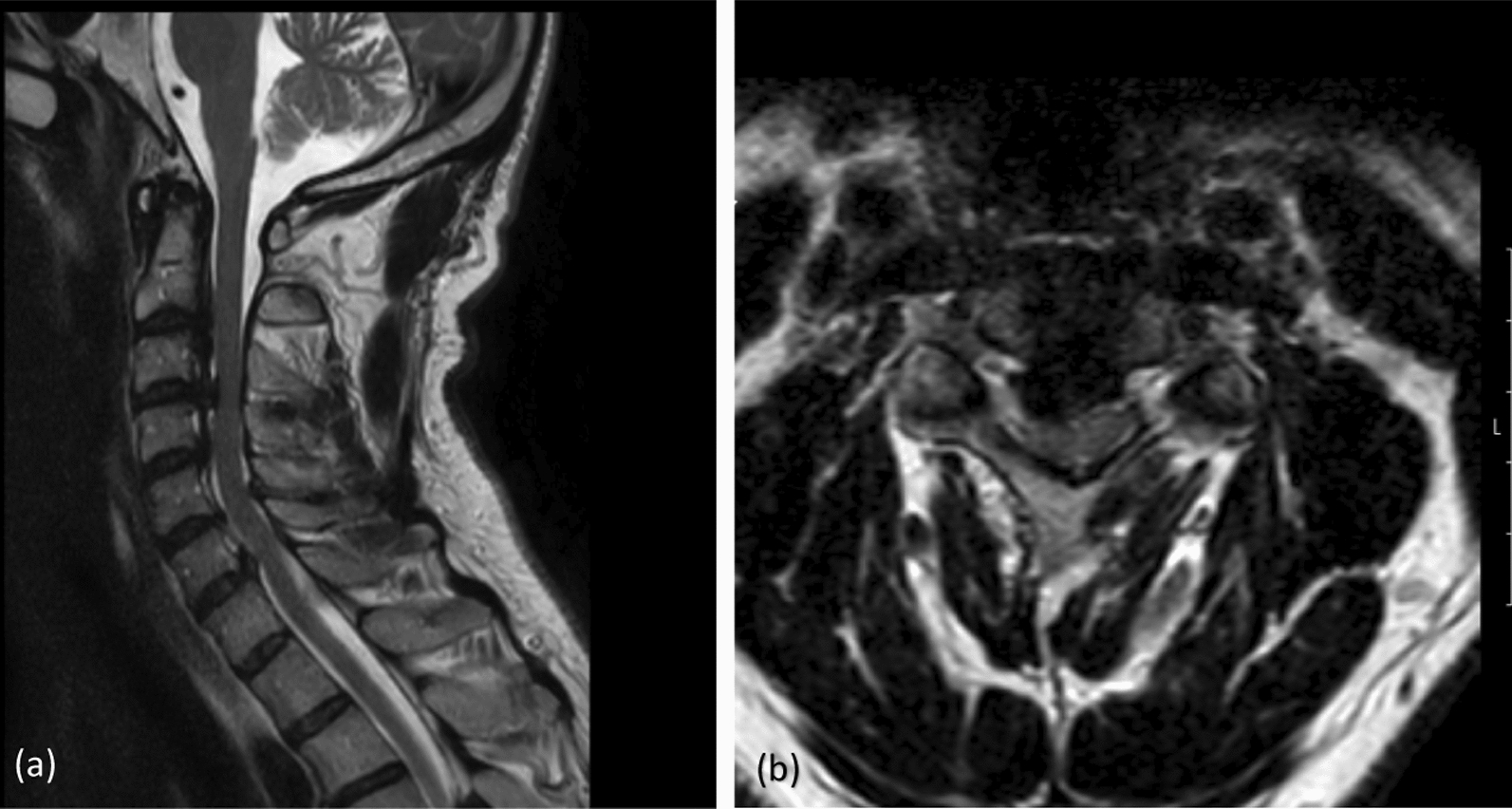
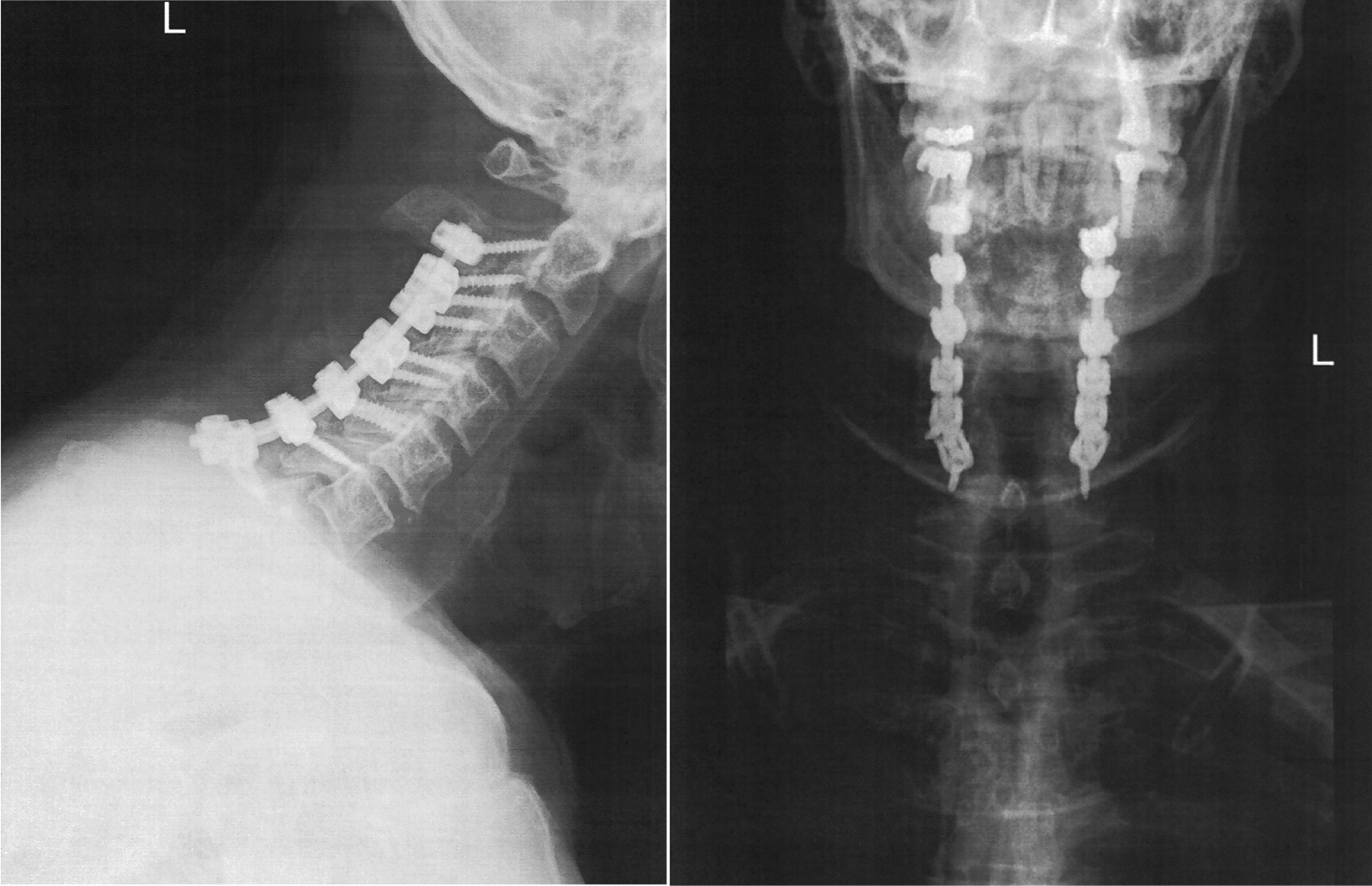
A 54-year-old Jewish male patient was diagnosed with disc herniation among the intervertebral discs at C2, C3, C4, C6, and C7, along with ossification of the posterior longitudinal ligament, pressuring more to the right side of the spinal canal, ruling-out cervical myelopathy. Under general anesthesia and multimodal intraoperative monitoring, he underwent laminectomy surgery from C3 to C6 and cervical fixation from C3 to C7. No blood pressure fluctuations occurred during surgery, and complete pressure release was achieved on the spinal cord and the nerve roots. In addition, neuromonitoring did not indicate any nerve damage during the surgery. A neurologic exam in the post-anesthesia care unit revealed weakness in his right hand and leg. A brain computed tomography scan ruled out cerebrovascular accident, neck computed tomography revealed optimal implant position, and magnetic resonance imaging ruled out spinal cord distress or injury. We treated him with intravenous fluids, steroids, painkillers, and anticoagulants. Following surgery, we involved the occupational therapy department. After a few days, we observed a significant improvement in motor function in the right leg; however, there was no change in the right hand.
White cord syndrome likely arises from reperfusion injury subsequent to surgical decompression of a compressed spinal cord segment. Although infrequent, it is imperative for spine surgeons to recognize this potential complication and apprise patients of it prior to the procedure.
脊髓缺血再灌注损伤的特征是神经功能突然下降,文献中仅有少数病例报道。本文报告了颈椎前路减压融合术后出现的“白索征”。
一名 54 岁犹太裔男性患者被诊断为 C2、C3、C4、C6 和 C7 椎间盘突出,同时存在后纵韧带骨化,向椎管右侧受压,排除了颈椎脊髓病。在全身麻醉和多模态术中监测下,患者接受了 C3 至 C6 的椎板切除术和 C3 至 C7 的颈椎固定术。手术过程中未出现血压波动,脊髓和神经根均实现了完全减压。此外,术中神经监测未显示任何神经损伤。麻醉后护理单元的神经检查显示右手和右腿无力。脑部计算机断层扫描排除了脑血管意外,颈部计算机断层扫描显示植入物位置理想,磁共振成像排除了脊髓受压或损伤。我们给予患者静脉输液、类固醇、止痛药和抗凝剂治疗。手术后,我们与职业治疗部门合作。几天后,我们观察到右腿运动功能明显改善,但右手无变化。
白索征可能是由于受压脊髓节段减压术后再灌注损伤引起的。尽管罕见,但脊柱外科医生必须认识到这种潜在的并发症,并在手术前告知患者。