Malone Daniel C, Biskupiak Joseph, Brixner Diana, Oderda Gary, Seheult Roger
College of Pharmacy, University of Utah, Salt Lake City, UT, USA.
University of California Riverside School of Medicine, Riverside, CA, and Loma Linda University School of Medicine, Loma Linda, CA, USA.
Am J Health Syst Pharm. 2025 Apr 29;82(9):e438-e446. doi: 10.1093/ajhp/zxae318.
COVID-19 patients in intensive care units (ICUs) requiring invasive mechanical ventilation (IMV) have few available treatment options. PANAMO, a multicenter, double-blind, randomized, placebo-controlled phase 3 study of vilobelimab, which blocks the inflammatory process caused by complement component 5a, demonstrated a significant mortality benefit at 28 and 60 days in these patients. A cost-effectiveness analysis was conducted to assess the incremental cost per quality-adjusted life-year (QALY).
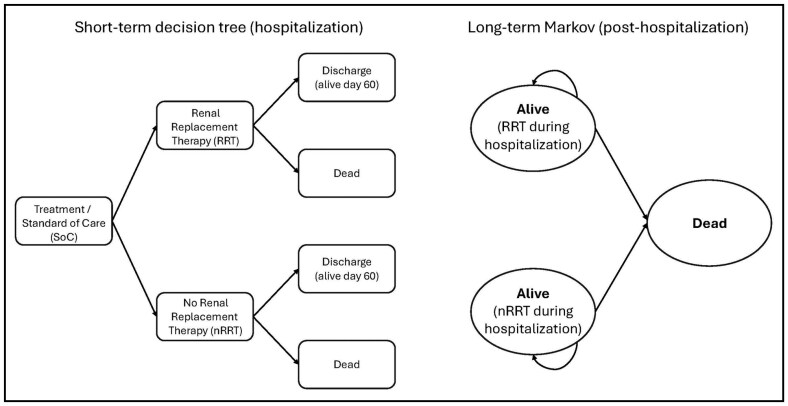
A Markov model was used to estimate QALYs and the incremental cost-effectiveness ratio (ICER) of vilobelimab plus standard of care (SOC) versus SOC alone. The model simulated progression from severe COVID-19 to survival or death over a lifetime horizon. Outcomes data (COVID-19 all-cause mortality and renal replacement therapy) were incorporated from the PANAMO trial. COVID-19 mortality estimates were based on Centers for Disease Control and Prevention age-specific survival data. Utility values and hospital costs came from the literature. Vilobelimab cost was obtained from RED BOOK Online.
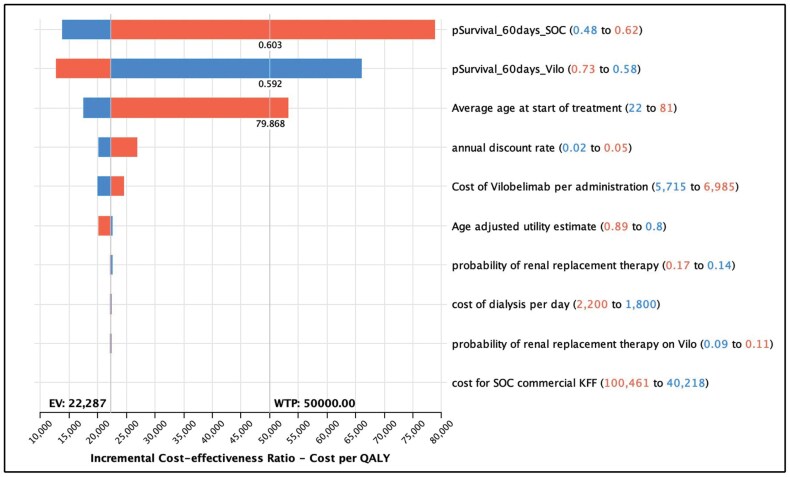
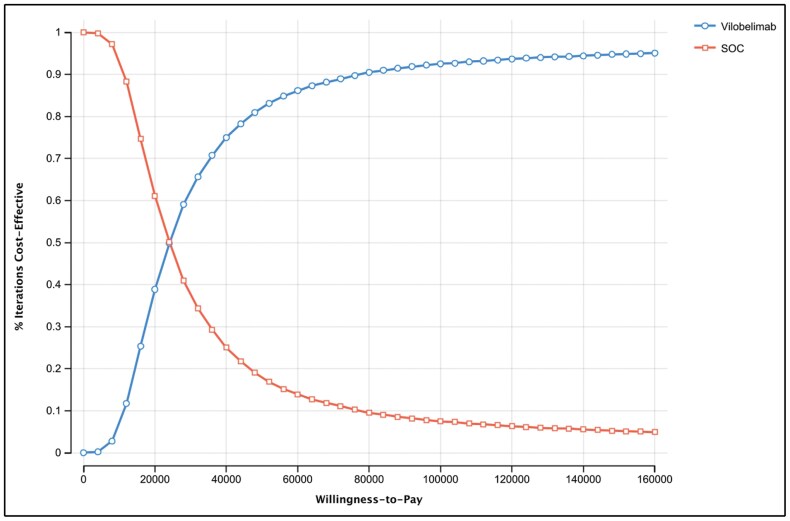
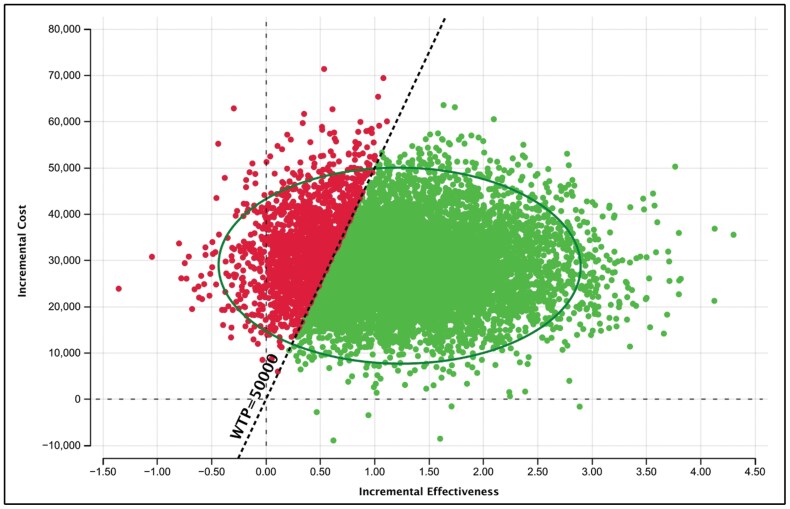
For COVID-19 ICU patients, total costs of care were $103,414 (SOC) and $132,247 (SOC plus vilobelimab), respectively, resulting in an incremental cost of $28,833. SOC provided 6.70 QALYs versus 7.99 QALYs for vilobelimab, an additional 1.29 QALYs. The ICER for vilobelimab plus SOC versus SOC alone was $22,287/QALY. Probabilistic sensitivity analysis demonstrated the robustness of the cost-effectiveness result as vilobelimab plus SOC was favored at a willingness-to-pay threshold of $50,000 in over 81% of iterations.
Vilobelimab provides a cost-effective option to treat ICU patients with severe COVID-19 receiving IMV compared to SOC, at well below the commonly accepted $50,000 US willingness-to-pay threshold.
需要有创机械通气(IMV)的重症监护病房(ICU)中的新冠肺炎患者可用的治疗选择很少。PANAMO是一项多中心、双盲、随机、安慰剂对照的3期研究,研究对象为可阻断补体成分5a引起的炎症过程的vilobelimab,该研究表明,在这些患者中,vilobelimab在28天和60天时具有显著的降低死亡率的益处。进行了一项成本效益分析,以评估每质量调整生命年(QALY)的增量成本。
使用马尔可夫模型来估计QALY以及vilobelimab加标准治疗(SOC)与单独使用SOC的增量成本效益比(ICER)。该模型模拟了从重症新冠肺炎到终身生存或死亡的进展情况。纳入了PANAMO试验的结果数据(新冠肺炎全因死亡率和肾脏替代治疗)。新冠肺炎死亡率估计基于疾病控制和预防中心的年龄特异性生存数据。效用值和医院成本来自文献。Vilobelimab成本从RED BOOK Online获得。
对于新冠肺炎ICU患者,护理总成本分别为103,414美元(SOC)和132,247美元(SOC加vilobelimab),增量成本为28,833美元。SOC提供了6.70个QALY,而vilobelimab为7.99个QALY,额外增加了1.29个QALY。vilobelimab加SOC与单独使用SOC的ICER为22,287美元/QALY。概率敏感性分析表明了成本效益结果的稳健性,因为在超过81%的迭代中,在支付意愿阈值为50,000美元时,vilobelimab加SOC更受青睐。
与SOC相比,vilobelimab为接受IMV的重症新冠肺炎ICU患者提供了一种具有成本效益的治疗选择,远低于普遍接受的50,000美元的美国支付意愿阈值。