Keller Michael, Acho Megan, Sun Junfeng, Kriner Eric, Seam Nitin, Lee Burton W
Critical Care Medicine Department, National Institutes of Health Clinical Center, National Heart, Lung, and Blood Institute, Bethesda, Maryland.
Department of Pulmonary Critical Care Medicine, Johns Hopkins Hospital, Baltimore, Maryland.
ATS Sch. 2024 Oct 30;5(2):302-310. doi: 10.34197/ats-scholar.2023-0051IN. eCollection 2024 Jun 1.
Prior evidence suggests that critical care trainees and attendings may have trouble recognizing common, potentially life-threatening mechanical ventilation (MV) waveform asynchronies. Although dedicated workshops may improve knowledge in MV, this knowledge may be prone to decay over time. Longitudinal, preceptorial-based curriculums may prevent this decay in knowledge.
To determine if the addition of a year-long, longitudinal MV preceptorial curriculum to a two-part, small-group, simulation-based education block curriculum reduces decay in MV knowledge compared with the education block curriculum alone.
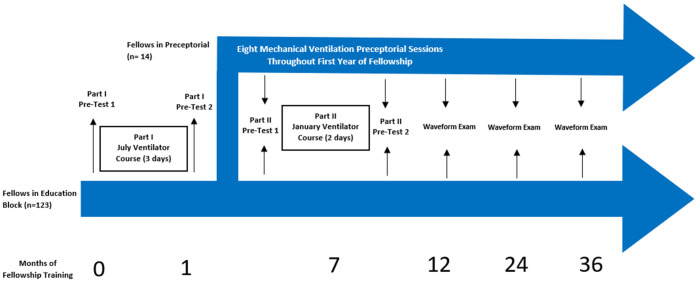
This was a multicenter prospective cohort study including 123 first-year fellows from 12 critical care fellowship programs who completed a two-part simulation-based education block (control) after the first and sixth months of fellowship. Fellows from one of these programs also participated in a year-long preceptorial curriculum (intervention). MV waveform examination scores over time during fellowship were compared between control versus intervention groups.
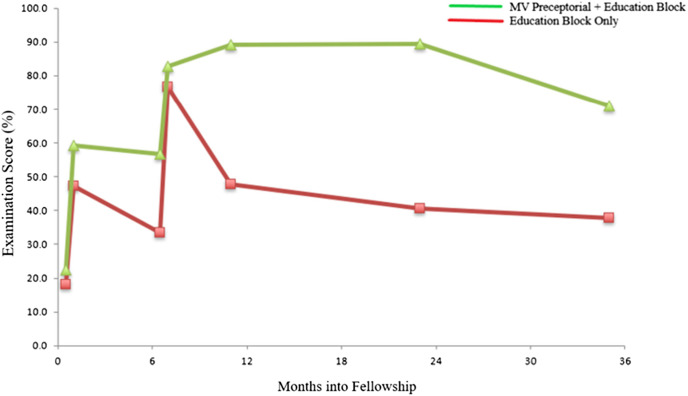
Mean test scores increased for both control and intervention groups after the education block courses at Months 1 and 6 of fellowship. Mean (standard deviation) test scores at Month 12 were higher for the intervention group than the control group (89.3 [14.8] vs. 47.7 [21.4]; < 0.0001). Between 6 months and 3 years of fellowship, there was a significant decay in test scores for the control group (slope estimate [standard error], -13.4 [1.7]; < 0.0001). However, there was no significant decay in test scores for the intervention group (slope estimate, -2.0 [4.7]; = 0.67; difference in slope estimates, 11.4 [5.0]; = 0.02).
The ability of critical care fellows to identify MV waveform asynchronies declines over fellowship training, despite a dedicated two-part, simulation-based MV educational curriculum. The addition of an MV preceptorial course decreased decay of MV knowledge over the course of fellowship training.
先前的证据表明,重症监护培训学员和主治医生可能难以识别常见的、可能危及生命的机械通气(MV)波形不同步情况。尽管专门的研讨会可能会提高对机械通气的认识,但随着时间的推移,这种认识可能会衰退。基于导师指导的纵向课程可能会防止这种知识衰退。
确定在一个由两部分组成的、基于小组模拟的教育模块课程基础上,增加为期一年的纵向MV导师指导课程,与仅采用教育模块课程相比,是否能减少MV知识的衰退。
这是一项多中心前瞻性队列研究,纳入了来自12个重症监护 fellowship 项目的123名第一年研究员,他们在 fellowship 的第一个月和第六个月后完成了一个由两部分组成的基于模拟的教育模块(对照组)。其中一个项目的研究员还参加了为期一年的导师指导课程(干预组)。比较了对照组和干预组在 fellowship 期间随时间变化的MV波形检查分数。
在 fellowship 的第1个月和第6个月的教育模块课程后,对照组和干预组的平均测试分数均有所提高。干预组在第12个月的平均(标准差)测试分数高于对照组(89.3 [14.8] 对 47.7 [21.4];<0.0001)。在 fellowship 的6个月至3年期间,对照组的测试分数有显著下降(斜率估计值 [标准误差],-13.4 [1.7];<0.0001)。然而,干预组的测试分数没有显著下降(斜率估计值,-2.0 [4.7];=0.67;斜率估计值差异,11.4 [5.0];=0.02)。
尽管有专门的由两部分组成的基于模拟的MV教育课程,但重症监护 fellowship 学员识别MV波形不同步的能力在 fellowship 培训期间仍会下降。增加MV导师指导课程可减少 fellowship 培训期间MV知识的衰退。