Kilić Domagoj, Peršić-Kiršić Sanja, Čelebić Asja
School of Dental Medicine, University of Zagreb, Gundulićeva 5 10000, Zagreb, Croatia.
Department of Removable Prosthodontics, School of Dental Medicine, University of Zagreb, Zagreb, Croatia.
Case Rep Dent. 2024 Oct 24;2024:4662194. doi: 10.1155/2024/4662194. eCollection 2024.
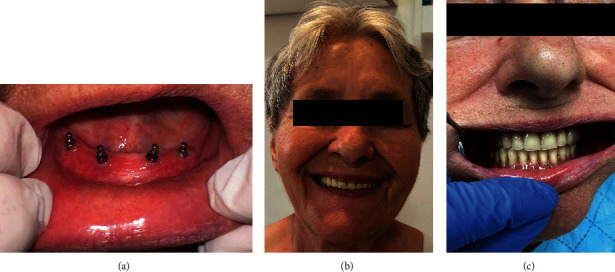
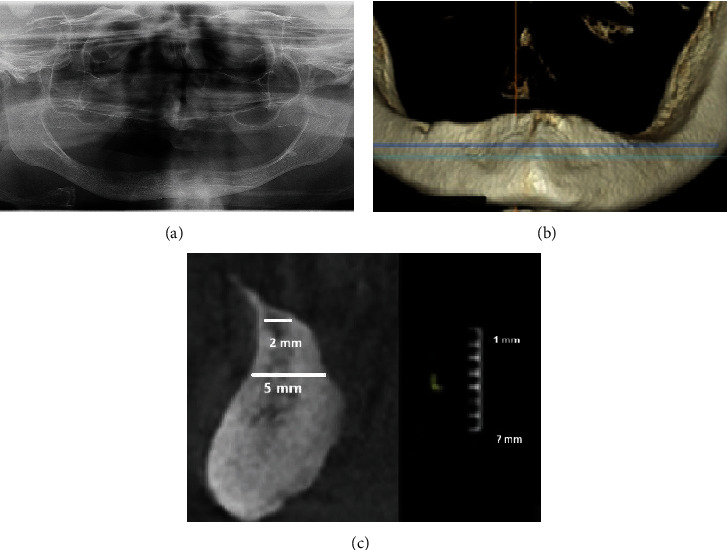
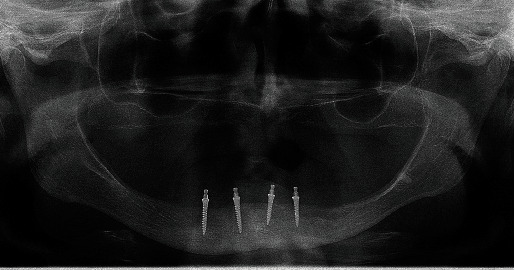
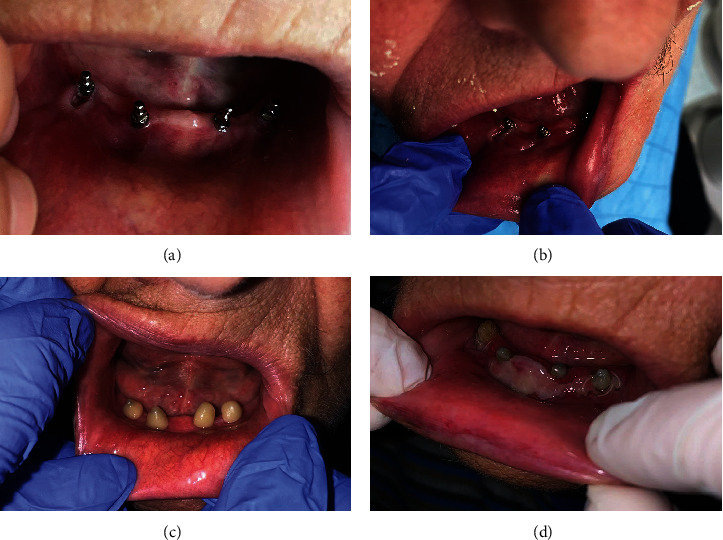
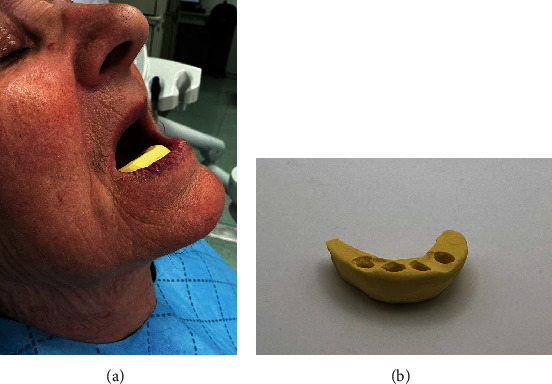
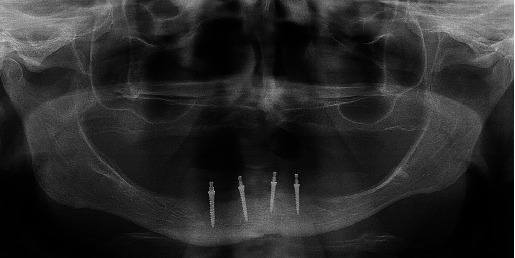
This clinical report describes how a decubital ulcer arose from the direct contact of the vestibular movable mucous membrane against mini-implant balled-type heads after the mini-implant insertion in the edentulous atrophic mandible of a 78-year-old patient who was not wearing a conventional mandibular complete denture for more than 10 years. Due to severe alveolar ridge atrophy, mini-implant insertion (2.0 mm wide) was an option without extensive surgical procedures. The patient signed the informed consent. A few days after the implant insertion, injury, inflammation, and induration of the vestibular movable mucous membrane were observed on the movable vestibular mucosa on the right side, opposing the mini-implants. The cause of inflammation was attributed to increased perioral muscle tonus which pushed the movable mucosa onto the mini-implant heads and caused mechanical trauma. During the period of edentulism, the perioral muscle tonus increased, directing the mucous membrane of the lips and cheeks against residual ridge to enable food comminution. To treat the persistent decubitus, a bulk of dental composite resin was placed around mini-implant heads and light-cured to protect the mucosa from further mechanical trauma, as the patient did not possess an old mandibular denture to cover the mini-implant heads. Vestibuloplastic surgery (disinsertion of movable attachments and deepening of the vestibulum) was also done. After the surgery, a silicone splint, resembling an occlusal rim, was made to protect the mucous membrane, keep medicaments for faster epitalization in place, to decrease perioral muscle tonus before the new dentures' delivery, and to prevent movable tissue relapse. The custom impression, jaw relationship determination, and try-in of the artificial teeth setup were made with sutures still in place. After the denture delivery and implant loading, the patient was instructed to sleep with the dentures to protect the movable mucous membrane. One year later, almost no peri-implant marginal bone loss was observed, attached and peri-implant mucosa were healthy, and the patient was delighted.
本临床报告描述了一名78岁无牙萎缩下颌患者,在未佩戴传统下颌全口义齿超过10年后,微型种植体植入无牙萎缩下颌后,前庭可移动黏膜与微型种植体球头直接接触如何引发褥疮性溃疡。由于严重的牙槽嵴萎缩,植入宽度为2.0毫米的微型种植体是一种无需广泛外科手术的选择。患者签署了知情同意书。种植体植入几天后,在与微型种植体相对的右侧可移动前庭黏膜上观察到前庭可移动黏膜的损伤、炎症和硬结。炎症原因归因于口周肌肉张力增加,将可移动黏膜推向微型种植体头部并造成机械性创伤。在无牙期,口周肌肉张力增加,使嘴唇和脸颊的黏膜抵靠残余牙槽嵴,以便粉碎食物。为治疗持续性褥疮,在微型种植体头部周围放置大量牙科复合树脂并光固化,以保护黏膜免受进一步的机械性创伤,因为患者没有旧的下颌义齿来覆盖微型种植体头部。还进行了前庭成形手术(松解可移动附着体并加深前庭)。手术后,制作了一个类似咬合缘的硅胶夹板,以保护黏膜,固定促进上皮化更快进行的药物,在新义齿交付前降低口周肌肉张力,并防止可移动组织复发。在缝线仍在位的情况下进行了定制印模、颌关系确定和人工牙排列试戴。义齿交付和种植体加载后,指导患者佩戴义齿睡觉以保护可移动黏膜。一年后,几乎未观察到种植体周围边缘骨丢失,附着的和种植体周围黏膜健康,患者很高兴。