Fasehun Oyinlola O, Adjei-Mensah Joycelyn, Ugorji Wisdom S, Titus Victoria O, Asade Oluwatobi O, Adeyemo Damilola A, Okobi Okelue E
Internal Medicine, University of Texas Rio Grande Valley, Weslaco, USA.
Internal Medicine, Achimota Hospital, Achimota, GHA.
Cureus. 2024 Oct 3;16(10):e70754. doi: 10.7759/cureus.70754. eCollection 2024 Oct.
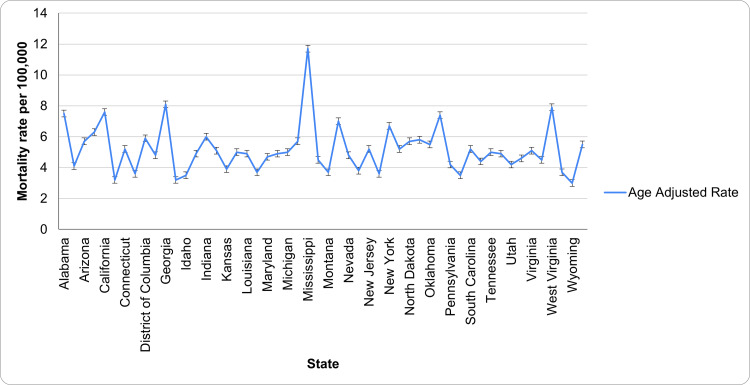
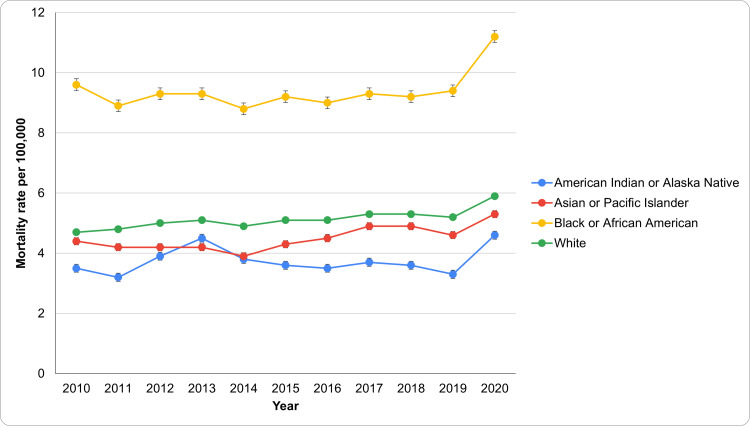
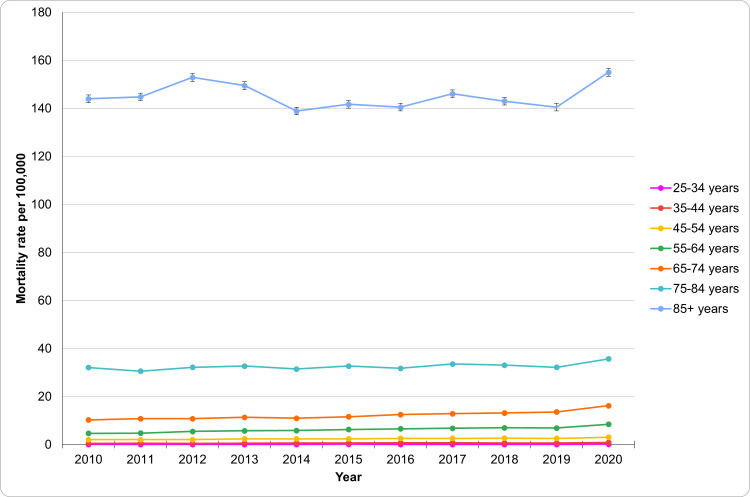
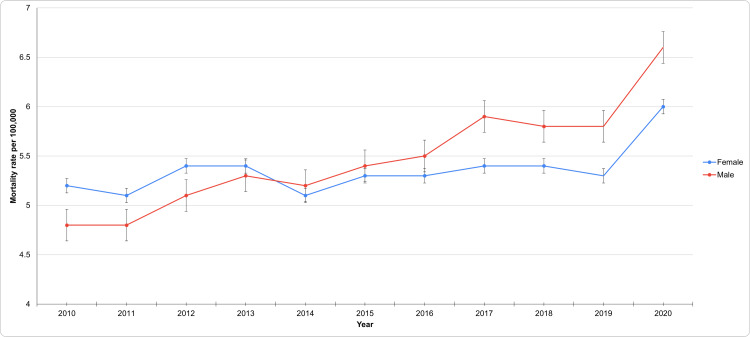
Hypertension (HTN) is a leading cause of cardiovascular morbidity and mortality worldwide. Despite advances in treatment, including the development and use of vasodilator-β-blocker combination and treatment with antihypertensive agents, HTN-related deaths have shown concerning trends. As such, the objective of this study is to examine the trends, disparities, and demographic variations in HTN-related mortality over a decade and to identify key factors contributing to these patterns, including genetics, dietary habits, structural discrimination in access to healthcare, lifestyle choices, and secondary hypertension, which is due to underlying conditions like kidney disease, hormonal disorders, or certain medications. To attain this objective, this retrospective study has utilized data from the Center for Disease Control and Prevention's Wide-Ranging Online Data for Epidemiologic Research (CDC WONDER) database to assess HTN-related mortality rates from 2010 to 2020. Age-adjusted mortality rates were calculated, and subgroup analyses were conducted by gender, race/ethnicity, and age groups. Temporal trends were analyzed to identify significant changes in mortality rates over time. Moreover, IBM SPSS Statistics, version 29 (IBM Corp., Armonk, NY) was used in the analysis, while 95% confidence intervals (CIs), were calculated to demonstrate the temporary trend of mortality rates overall and by age, sex, ethnicity, and region. Therefore, the mortality data from 2010 to 2020 show significant trends and variations across demographic groups. Overall, HTN-related mortality rate in the United States increased from 5.1 per 100,000 in 2010 to 6.4 in 2020, reflecting a general upward trend. For males, the rate rose from 4.8 to 6.6 per 100,000 during the same period. Racial disparities are notable, with Black or African American individuals having the highest mortality rates, increasing from 9.6 to 11.2 per 100,000. Age-specific data reveal that mortality in the 65-74 age group more than doubled, from 10.3 to 16.2 per 100,000, while in the 75-84 age group, it rose from 32.1 to 35.7. The 85+ age group had the highest rates, increasing from 144.0 to 155.0 per 100,000. States with the highest age-adjusted rates include Mississippi, Georgia, West Virginia, California, and Alabama. The study findings highlight the growing burden of HTN-related mortality in the United States, particularly among males, racial minorities, and older adults. This situation underscores the need for targeted public health interventions, which include creation of hypertension awareness in minority groups and enhancing medication adherence especially among Blacks, and addressing the social determinants of health contributing to higher HTN rates and poorer outcomes, including disadvantaged neighborhoods, structural discrimination and racism, and limited access to healthcare. The study found that African Americans are likely to be diagnosed with HTN earlier in life with higher HTN-related mortality than Whites, and with 50% increased risk of cardiovascular disease mortality. Continuous efforts are required to aptly address such disparities contributing to ongoing HTN treatment and care inequalities.
高血压(HTN)是全球心血管疾病发病和死亡的主要原因。尽管在治疗方面取得了进展,包括血管扩张剂-β受体阻滞剂组合的开发和使用以及抗高血压药物治疗,但与高血压相关的死亡呈现出令人担忧的趋势。因此,本研究的目的是考察十年来与高血压相关的死亡率的趋势、差异和人口统计学变化,并确定导致这些模式的关键因素,包括遗传、饮食习惯、获得医疗保健方面的结构性歧视、生活方式选择以及继发性高血压,继发性高血压是由肾脏疾病、激素紊乱或某些药物等潜在疾病引起的。为实现这一目标,这项回顾性研究利用了疾病控制和预防中心的广泛在线流行病学研究数据(CDC WONDER)数据库来评估2010年至2020年与高血压相关的死亡率。计算了年龄调整后的死亡率,并按性别、种族/族裔和年龄组进行了亚组分析。分析了时间趋势,以确定死亡率随时间的显著变化。此外,分析中使用了IBM SPSS Statistics 29版(IBM公司,纽约州阿蒙克),同时计算了95%置信区间(CIs),以展示总体死亡率以及按年龄、性别、种族和地区划分的死亡率的时间趋势。因此,2010年至2020年的死亡率数据显示了不同人口群体之间的显著趋势和差异。总体而言,美国与高血压相关的死亡率从2010年的每10万人5.1例增加到2020年的6.4例,呈现出总体上升趋势。男性的死亡率在同一时期从每10万人4.8例上升到6.6例。种族差异显著,黑人或非裔美国人的死亡率最高,从每10万人9.6例增加到11.2例。特定年龄数据显示,65 - 74岁年龄组的死亡率增加了一倍多,从每10万人10.3例增加到16.2例,而在75 - 84岁年龄组,死亡率从32.1例上升到35.7例。85岁及以上年龄组的死亡率最高,从每10万人144.0例增加到155.0例。年龄调整率最高的州包括密西西比州、佐治亚州、西弗吉尼亚州、加利福尼亚州和阿拉巴马州。研究结果凸显了美国与高血压相关的死亡率负担日益加重,尤其是在男性、少数族裔和老年人中。这种情况强调了有针对性的公共卫生干预措施的必要性,这些措施包括在少数群体中提高高血压意识,特别是提高黑人的药物依从性,以及解决导致高血压发病率较高和预后较差的健康的社会决定因素,包括处境不利的社区、结构性歧视和种族主义以及获得医疗保健的机会有限。研究发现,非裔美国人比白人更可能在生命早期被诊断出患有高血压,且与高血压相关的死亡率更高,心血管疾病死亡风险增加50%。需要持续努力以妥善解决这些导致高血压治疗和护理不平等持续存在的差异。