Cai Jennifer, Fernandez-Hazoury David, Yoshikawa Gene, Minja Amani, Huang Hehua, Hwang Andrew, Qing Xin
Department of Pathology, Harbor-UCLA Medical Center, Torrance, CA 90502, USA.
University of California at Irvine, Irvine, CA, USA.
J Hematol. 2024 Oct;13(5):216-223. doi: 10.14740/jh1310. Epub 2024 Sep 16.
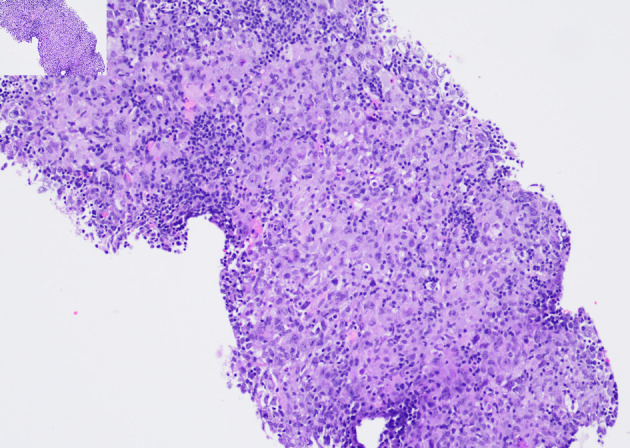
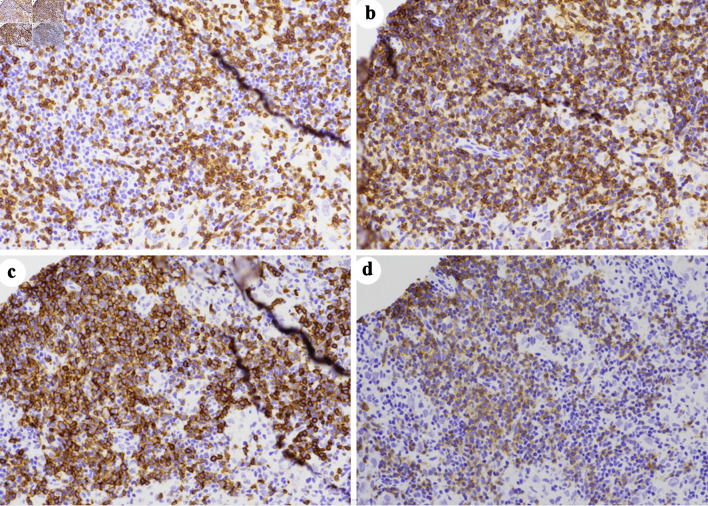
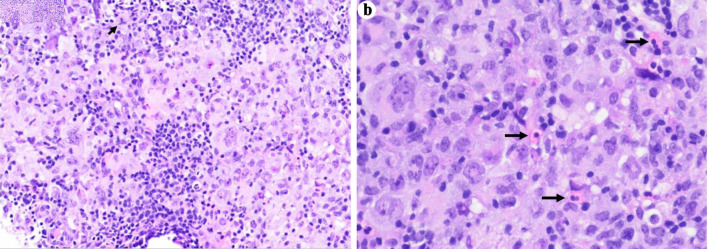
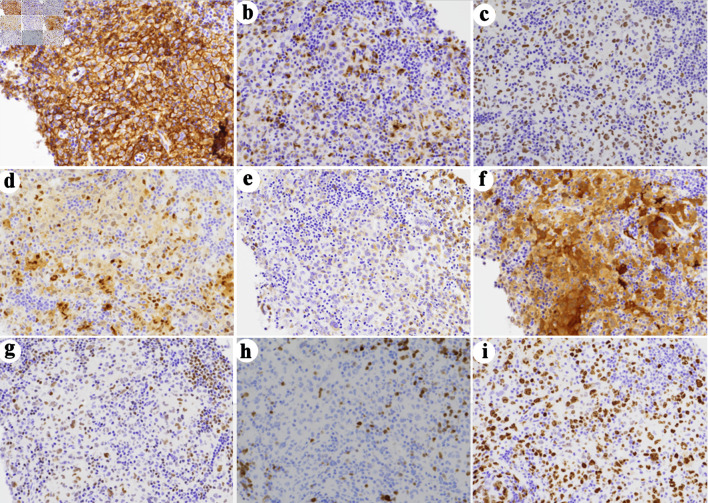
Chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) transforming into a more aggressive lymphoma (i.e., Richter syndrome) is well documented in the literature. In recent years, transdifferentiation of CLL/SLL to histiocytic/dendritic/Langerhans cell sarcomas has also been reported. We hereby describe a case of a 55-year-old female who was incidentally diagnosed with CLL after presenting to the hospital for symptoms of undiagnosed rheumatoid arthritis. At the time of presentation, CLL was stage 1, and the patient was placed on observation. Eight years after being diagnosed with CLL, and after several treatment modalities for her rheumatoid arthritis, the patient re-presented with progression of adenopathy, intermittent fevers, 5-pound weight loss, and worsening respiratory status requiring airway management. Computed tomography (CT) imaging revealed a soft tissue mass in the nasopharynx, lingual tonsillar hypertrophy with airway compromise, and bulky cervical, supraclavicular, and axillary lymphadenopathy. A biopsy of an enlarged cervical lymph node yielded a diagnosis of histiocytic/dendritic cell sarcoma favoring interdigitating dendritic cell sarcoma, likely representing transdifferentiation from CLL/SLL, of which there are no standard of care treatment guidelines. The patient was treated with ifosfamide, carboplatin, and etoposide (ICE) for three cycles, followed by rituximab, etoposide, prednisone, vincristine, cyclophosphamide, and doxorubicin (R-EPOCH) in combination with zanubrutinib. She then underwent haploidentical hematopoietic stem cell transplantation. At the time of the making of this manuscript, the patient was 45 days post-transplant without any notable complications.
慢性淋巴细胞白血病/小淋巴细胞淋巴瘤(CLL/SLL)转化为侵袭性更强的淋巴瘤(即里氏综合征)在文献中有充分记载。近年来,也有报道称CLL/SLL可转分化为组织细胞/树突状/Langerhans细胞肉瘤。我们在此描述一例55岁女性病例,该患者因未确诊的类风湿性关节炎症状入院,偶然被诊断为CLL。就诊时,CLL处于1期,患者接受观察。在被诊断为CLL八年后,且在对其类风湿性关节炎进行了多种治疗后,患者再次出现淋巴结病进展、间歇性发热、体重减轻5磅以及呼吸状况恶化需要气道管理。计算机断层扫描(CT)成像显示鼻咽部有软组织肿块、舌扁桃体肥大伴气道受压,以及颈部、锁骨上和腋窝淋巴结肿大。对一个肿大的颈部淋巴结进行活检,诊断为组织细胞/树突状细胞肉瘤,倾向于指状突树突状细胞肉瘤,可能代表CLL/SLL的转分化,对此尚无标准的治疗指南。患者接受了三个周期的异环磷酰胺、卡铂和依托泊苷(ICE)治疗,随后接受利妥昔单抗、依托泊苷、泼尼松、长春新碱、环磷酰胺和多柔比星(R-EPOCH)联合泽布替尼治疗。然后她接受了单倍体造血干细胞移植。在撰写本手稿时,患者移植后45天,无任何明显并发症。