Stewart Tyler F, Chalfin Healther, Simon Nicholas, Tan Alan, Apolo Andrea, McKay Rana R
Department of Medicine, University of California San Diego, La Jolla, CA, USA.
National Cancer Institute, NIH, Bethesda, MD, USA.
Bladder Cancer. 2024 Oct 23;10(3):183-198. doi: 10.3233/BLC-230105. eCollection 2024.
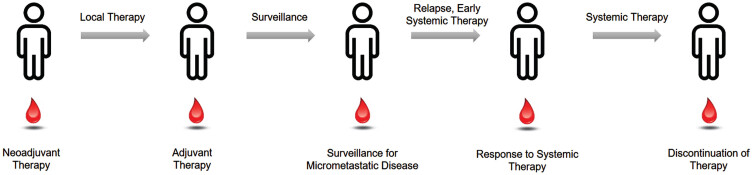
Muscle-invasive bladder cancer represents a potentially curable disease, yet often disease recurs and is ultimately fatal. Outcomes for patients with localized urothelial carcinoma are heterogeneous with some patients cured with surgery alone, deriving no benefit from perioperative systemic therapy, while others are left with residual disease and may benefit from additional therapy. Neoadjuvant chemotherapy increases cure rates but comes with significant toxicity. Recently, adjuvant nivolumab has demonstrated significant improvement in disease free survival (DFS), and overall survival analysis is pending. With more therapies approved for urothelial cancer within the last 5 years than ever before, there is incredible potential to improve clinical outcomes and potentially cure more patients with integrated multimodal therapy. Biomarkers are needed to dichotomize those most likely to benefit from perioperative systemic therapy for residual disease, and de-escalate therapy for those likely to be cured with surgery alone. Ultrasensitive assays for circulating tumor DNA (ctDNA) have emerged as a method to identify patients at high risk of recurrence after definitive therapy and may benefit from escalated therapy, while also identifying those least likely to benefit from systemic therapy. Studies have demonstrated that the presence of ctDNA after surgery is prognostic of disease recurrence across multiple cancer types, including bladder cancer, but questions remain as to the utility of these tests, and whether they can be predictive of benefit of adjuvant therapy. Although these liquid biopsies hold significant promise to transform perioperative treatment, prospective studies are needed to validate their utility as prognostic and predictive biomarkers. To bridge this knowledge gap, contemporary clinical trials are incorporating ctDNA as an integral biomarker to guide therapy for MIBC.
肌肉浸润性膀胱癌是一种潜在可治愈的疾病,但疾病常复发并最终导致死亡。局限性尿路上皮癌患者的预后存在异质性,一些患者仅通过手术治愈,围手术期全身治疗并无益处,而另一些患者则留有残余疾病,可能从额外治疗中获益。新辅助化疗可提高治愈率,但伴有显著毒性。最近,辅助性纳武单抗已证明无病生存期(DFS)有显著改善,总生存分析正在进行中。在过去5年中,获批用于尿路上皮癌的治疗方法比以往任何时候都多,采用综合多模式治疗改善临床结局并潜在治愈更多患者的潜力巨大。需要生物标志物来区分那些最有可能从围手术期全身治疗中获益以治疗残余疾病的患者,并对那些可能仅通过手术治愈的患者降低治疗强度。循环肿瘤DNA(ctDNA)的超灵敏检测已成为一种方法,可识别根治性治疗后复发风险高且可能从强化治疗中获益的患者,同时也能识别那些最不可能从全身治疗中获益的患者。研究表明,手术后ctDNA的存在可预测包括膀胱癌在内的多种癌症类型的疾病复发,但这些检测的实用性以及它们是否能预测辅助治疗的获益仍存在疑问。尽管这些液体活检有望改变围手术期治疗,但仍需要前瞻性研究来验证其作为预后和预测生物标志物的效用。为了填补这一知识空白,当代临床试验正在将ctDNA作为一种不可或缺的生物标志物纳入其中,以指导肌肉浸润性膀胱癌的治疗。