Rocha Nazareth N, Silva Pedro L, Battaglini Denise, Rocco Patricia R M
Biomedical Institute, Department of Physiology and Pharmacology, Fluminense Federal University, Niteroi, Brazil.
Laboratory of Pulmonary Investigation, Carlos Chagas Filho Institute of Biophysics, Federal University of Rio de Janeiro, Rio de Janeiro, Brazil.
Front Physiol. 2024 Oct 18;15:1478514. doi: 10.3389/fphys.2024.1478514. eCollection 2024.
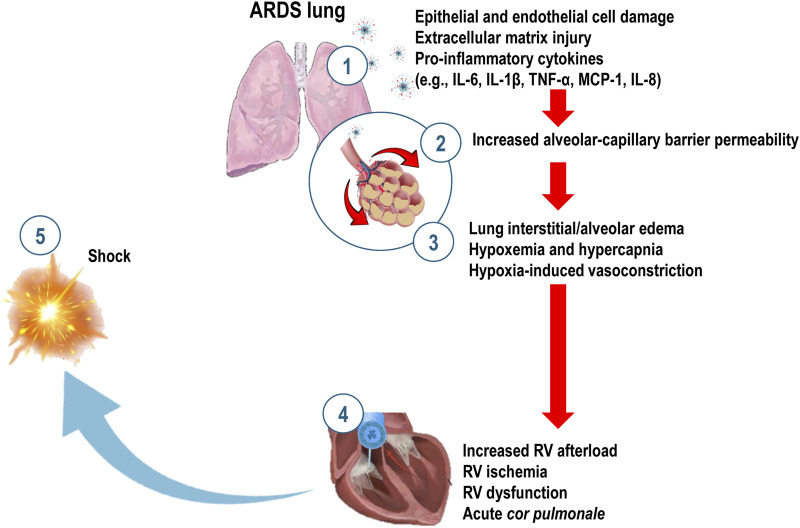
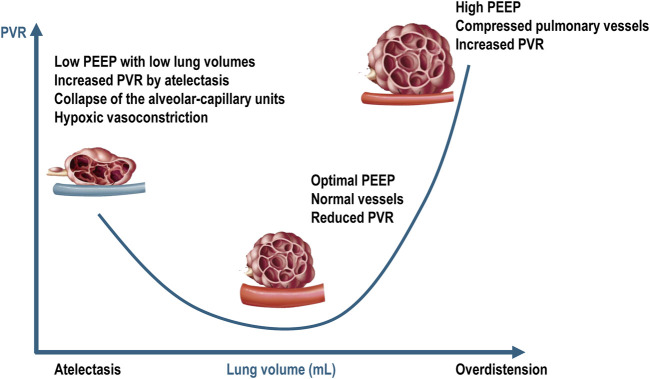
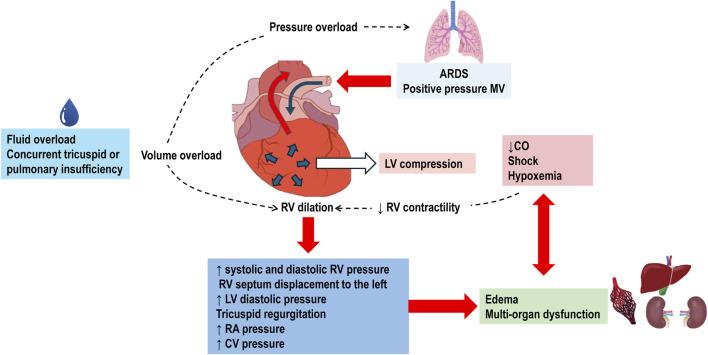
Acute Respiratory Distress Syndrome (ARDS) is initiated by a primary insult that triggers a cascade of pathological events, including damage to lung epithelial and endothelial cells, extracellular matrix disruption, activation of immune cells, and the release of pro-inflammatory mediators. These events lead to increased alveolar-capillary barrier permeability, resulting in interstitial/alveolar edema, collapse, and subsequent hypoxia and hypercapnia. ARDS not only affects the lungs but also significantly impacts the cardiovascular system. We conducted a comprehensive literature review on heart-lung crosstalk in ARDS, focusing on the pathophysiology, effects of mechanical ventilation, hypoxemia, and hypercapnia on cardiac function, as well as ARDS secondary to cardiac arrest and cardiac surgery. Mechanical ventilation, essential for ARDS management, can increase intrathoracic pressure, decrease venous return and right ventricle preload. Moreover, acidemia and elevations in transpulmonary pressures with mechanical ventilation both increase pulmonary vascular resistance and right ventricle afterload. Cardiac dysfunction can exacerbate pulmonary edema and impair gas exchange, creating a vicious cycle, which hinders both heart and lung therapy. In conclusion, understanding the heart-lung crosstalk in ARDS is important to optimize therapeutic strategies. Future research should focus on elucidating the precise mechanisms underlying this interplay and developing targeted interventions that address both organs simultaneously.
急性呼吸窘迫综合征(ARDS)由原发性损伤引发,该损伤会触发一系列病理事件,包括肺上皮细胞和内皮细胞损伤、细胞外基质破坏、免疫细胞激活以及促炎介质释放。这些事件导致肺泡-毛细血管屏障通透性增加,进而引起间质/肺泡水肿、肺萎陷,随后出现低氧血症和高碳酸血症。ARDS不仅影响肺部,还会对心血管系统产生重大影响。我们对ARDS中心肺相互作用进行了全面的文献综述,重点关注病理生理学、机械通气、低氧血症和高碳酸血症对心脏功能的影响,以及心脏骤停和心脏手术后继发的ARDS。机械通气是ARDS治疗的关键,它会增加胸内压,减少静脉回流和右心室前负荷。此外,机械通气导致的酸血症和跨肺压升高都会增加肺血管阻力和右心室后负荷。心脏功能障碍会加重肺水肿并损害气体交换,形成恶性循环,阻碍心肺治疗。总之,了解ARDS中的心肺相互作用对于优化治疗策略至关重要。未来的研究应专注于阐明这种相互作用的精确机制,并开发同时针对两个器官的靶向干预措施。