Schaafsma Mirte, Schuurman Teska N, Kootstra Pien, Issa Deli, Hermans Ivo, Bleeker Maaike C G, Zusterzeel Petra L M, Bekkers Ruud L M, Siebers Albert G, Mom Constantijne H, van Trommel Nienke E
Department of Gynecologic Oncology, Center of Gynecologic Oncology Amsterdam, Antoni van Leeuwenhoek/Netherlands Cancer Institute, Amsterdam, The Netherlands.
Department of Pathology, Amsterdam UMC, Vrije Universiteit Amsterdam, Amsterdam, The Netherlands.
Int J Cancer. 2025 Mar 15;156(6):1203-1212. doi: 10.1002/ijc.35237. Epub 2024 Nov 4.
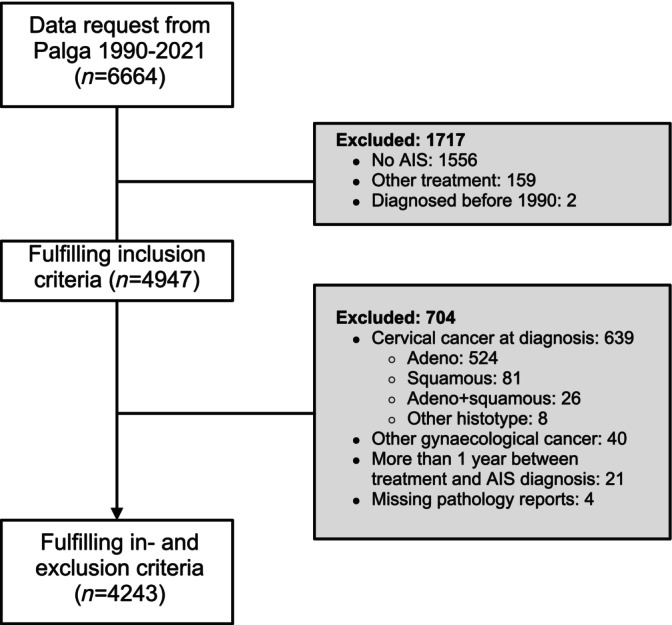
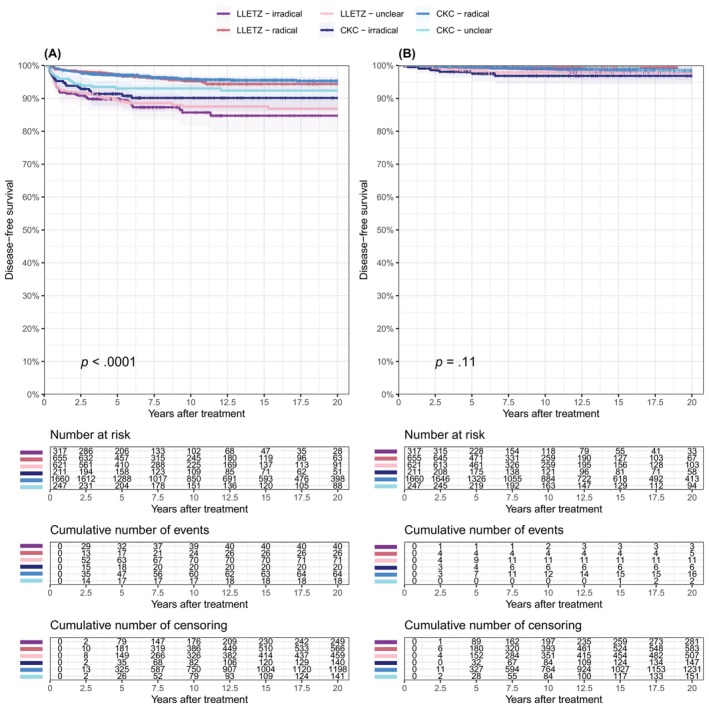
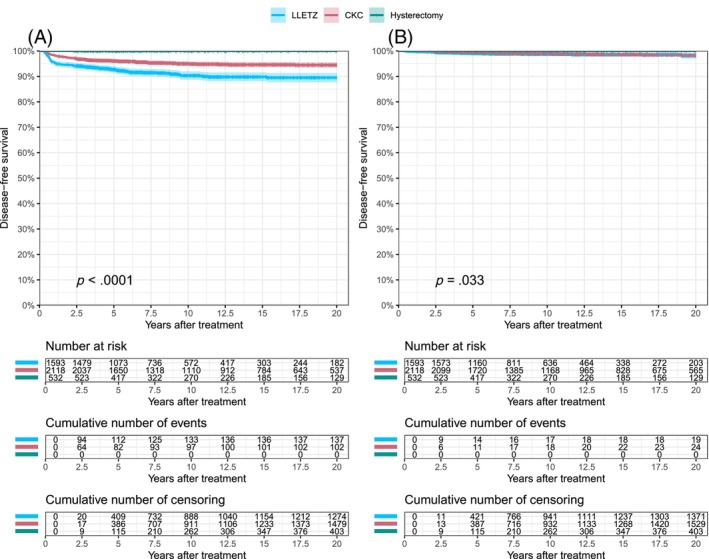
Internationally, little consensus exists about the best treatment for cervical adenocarcinoma in situ (AIS). This study aimed to determine the incidence of recurrent high-grade cervical dysplasia and development of local cervical cancer after treatment for AIS. This nationwide, retrospective cohort study included patients with AIS, who were treated by a large loop excision of the transformation zone (LLETZ), cold-knife conization (CKC), or hysterectomy between January 1, 1990 and December 31, 2021 in the Netherlands. Pathology reports were retrieved from the Dutch Nationwide Pathology Databank (Palga). Primary outcomes were the cumulative incidences of high-grade cervical dysplasia (cervical intraepithelial neoplasia grade 2 or 3, and AIS) and local cervical cancer up to 20 years after primary treatment. In total, 4243 patients with AIS were included. The primary treatment was a LLETZ, CKC, or hysterectomy in 1593, 2118, and 532 patients, respectively. The incidence of recurrent high-grade cervical dysplasia after LLETZ (10.5%; 95%CI: 8.6-12.3) was higher than after CKC (5.5%; 95%CI: 4.4-6.6, p <.0001). When a radical excision, that is, surgical margins free of dysplasia at end of treatment, was achieved, the incidence of recurrent high-grade dysplasia and local cervical cancer did not differ between LLETZ (5.6% [95%CI: 3.3-7.9] and 1.9% [95%CI: 0-4.4]) and CKC (4.7% [95%CI: 3.5-5.8], p = .631 and 1.5% [95%CI: 0.7-2.3], p = .918). After hysterectomy, none of the patients developed cervical dysplasia or local cervical cancer. Conservative treatment for AIS can be considered a safe and final treatment modality when a radical excision is achieved.
在国际上,对于宫颈原位腺癌(AIS)的最佳治疗方法,几乎没有达成共识。本研究旨在确定AIS治疗后高级别宫颈发育异常复发的发生率以及局部宫颈癌的发生情况。这项全国性的回顾性队列研究纳入了1990年1月1日至2021年12月31日期间在荷兰接受转化区大环状切除术(LLETZ)、冷刀锥切术(CKC)或子宫切除术治疗的AIS患者。病理报告从荷兰全国病理数据库(Palga)中获取。主要结局是初次治疗后20年内高级别宫颈发育异常(宫颈上皮内瘤变2级或3级以及AIS)和局部宫颈癌的累积发生率。总共纳入了4243例AIS患者。初次治疗分别为LLETZ、CKC或子宫切除术的患者有1593例、2118例和532例。LLETZ术后高级别宫颈发育异常复发的发生率(10.5%;95%置信区间:8.6 - 12.3)高于CKC术后(5.5%;95%置信区间:4.4 - 6.6,p <.0001)。当实现根治性切除,即治疗结束时手术切缘无发育异常时,LLETZ(5.6% [95%置信区间:3.3 - 7.9]和1.9% [95%置信区间:0 - 4.4])和CKC(4.7% [95%置信区间:3.5 - 5.8],p = 0.631和1.5% [95%置信区间:0.7 - 2.3],p = 0.918)术后高级别发育异常复发和局部宫颈癌的发生率没有差异。子宫切除术后,没有患者发生宫颈发育异常或局部宫颈癌。当实现根治性切除时,AIS的保守治疗可被视为一种安全的最终治疗方式。