Salomon Benita, Sudhakar Padhmanand, Bergemalm Daniel, Andersson Erik, Grännö Olle, Carlson Marie, Hedin Charlotte R H, Söderholm Johan D, Öhman Lena, Lindqvist Carl Mårten, Kruse Robert, Repsilber Dirk, Verstockt Bram, Vermeire Séverine, Halfvarson Jonas
Faculty of Medicine and Health, School of Medical Sciences, Örebro University, Örebro, Sweden.
Department of Chronic Diseases and Metabolism, Translational Research Center for Gastrointestinal Disorders (TARGID), KU Leuven, Leuven, Belgium.
J Crohns Colitis. 2025 May 8;19(5). doi: 10.1093/ecco-jcc/jjae169.
Recent genetic and transcriptomic data highlight the need for improved molecular characterization of inflammatory bowel disease (IBD). Proteomics may advance the delineation of IBD phenotypes since it accounts for post-transcriptional modifications.
We aimed to assess the IBD spectrum based on inflammatory serum proteins and identify discriminative patterns of underlying biological subtypes across multiple European cohorts.
Using proximity extension methodology, we measured 86 inflammation-related serum proteins in 1551 IBD patients and 312 healthy controls (HC). We screened for proteins exhibiting significantly different levels among IBD subtypes and between IBD and HC. Classification models for differentiating between Crohn's disease (CD) and ulcerative colitis (UC) were employed to explore the IBD spectrum based on estimated probability scores.
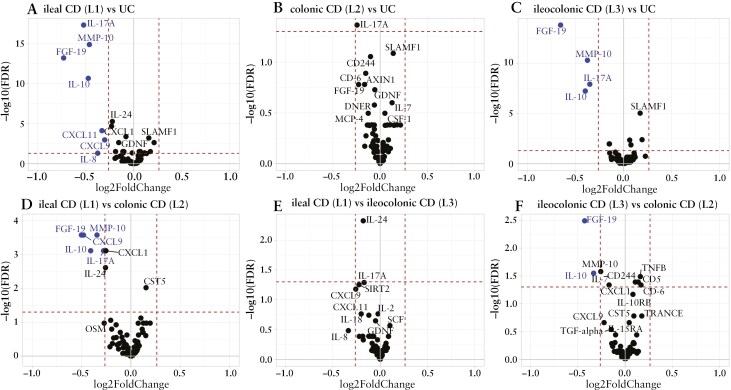
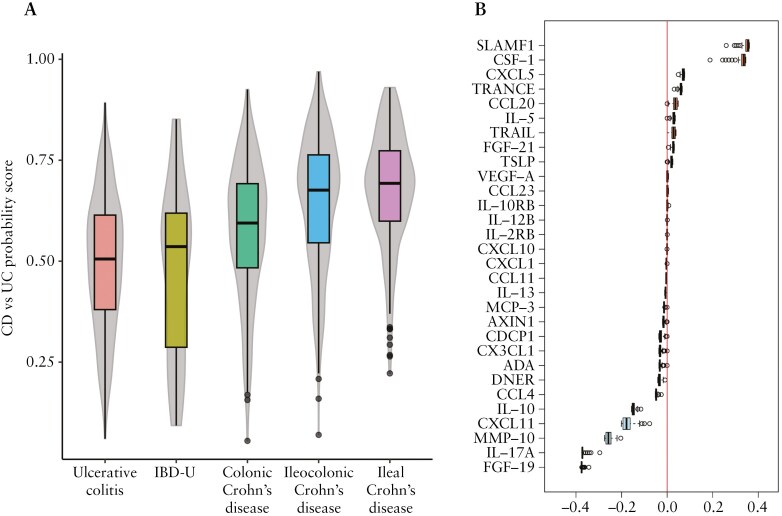
Levels of multiple proteins, such as interleukin-17A, matrix metalloproteinase-10, and fibroblast growth factor-19, differed (fold-change >1.2; false discovery rate <0.05) between ileal versus colonic IBD. Using multivariable models, a protein signature reflecting the IBD spectrum was identified, positioning colonic CD between UC and ileal CD, which were at opposite ends of the spectrum. Based on area under the curve (AUC) estimates, classification models more accurately differentiated UC from ileal CD (median AUCs > 0.73) than colonic CD (median AUCs < 0.62). Models differentiating colonic CD from ileal CD demonstrated intermediate performance (median AUCs: 0.67-0.69).
Our findings in serum proteins support the presence of a continuous IBD spectrum rather than a clear separation of CD and UC. Within the spectrum, disease location may reflect a more similar disease than CD versus UC, as colonic CD resembled UC more closely than ileal CD.
近期的基因和转录组数据凸显了改善炎症性肠病(IBD)分子特征描述的必要性。蛋白质组学可能会推动IBD表型的界定,因为它考虑了转录后修饰。
我们旨在基于炎症血清蛋白评估IBD谱,并在多个欧洲队列中识别潜在生物学亚型的判别模式。
使用邻近延伸法,我们测量了1551例IBD患者和312名健康对照(HC)中86种炎症相关血清蛋白。我们筛选了在IBD亚型之间以及IBD与HC之间表现出显著不同水平的蛋白质。采用区分克罗恩病(CD)和溃疡性结肠炎(UC)的分类模型,基于估计的概率分数探索IBD谱。
多种蛋白质的水平,如白细胞介素-17A、基质金属蛋白酶-10和成纤维细胞生长因子-19,在回肠型与结肠型IBD之间存在差异(倍数变化>1.2;错误发现率<0.05)。使用多变量模型,识别出了一个反映IBD谱的蛋白质特征,将结肠型CD定位在UC和回肠型CD之间,而UC和回肠型CD位于谱的两端。基于曲线下面积(AUC)估计,分类模型区分UC和回肠型CD(中位数AUCs>0.73)比区分结肠型CD(中位数AUCs<0.62)更准确。区分结肠型CD和回肠型CD的模型表现居中(中位数AUCs:0.67 - 0.69)。
我们在血清蛋白方面的发现支持存在连续的IBD谱,而非CD和UC的明确区分。在该谱内,疾病部位可能反映出比CD与UC更相似的疾病,因为结肠型CD比回肠型CD更类似于UC。