School of Health & Wellbeing, University of Glasgow, Glasgow, United Kingdom.
Clinical Research Department, London School of Hygiene & Tropical Medicine, London, United Kingdom.
PLoS Med. 2024 Nov 5;21(11):e1004448. doi: 10.1371/journal.pmed.1004448. eCollection 2024 Nov.
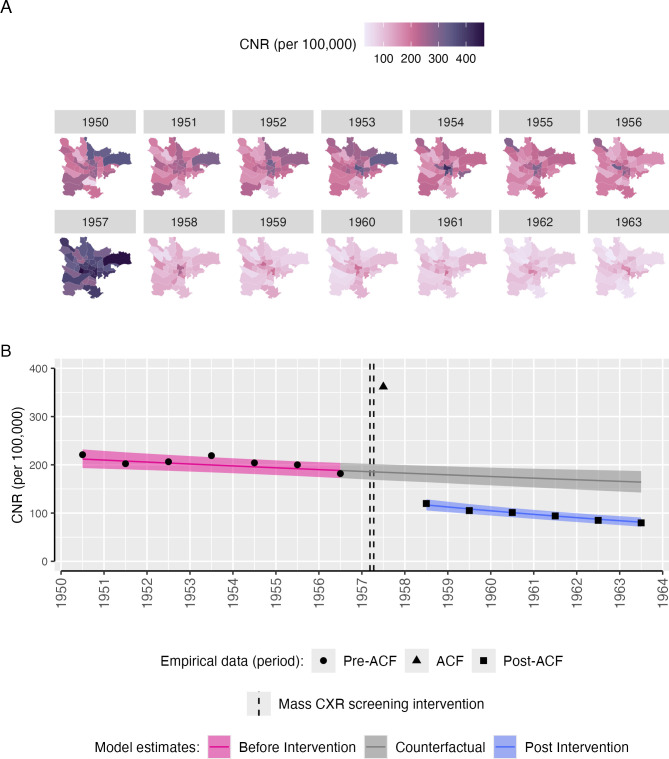
Community active case finding (ACF) for tuberculosis was widely implemented in Europe and North America between 1940 and 1970, when incidence was comparable to many present-day high-burden countries. Using an interrupted time series analysis, we analysed the effect of the 1957 Glasgow mass chest X-ray campaign to inform contemporary approaches to screening.
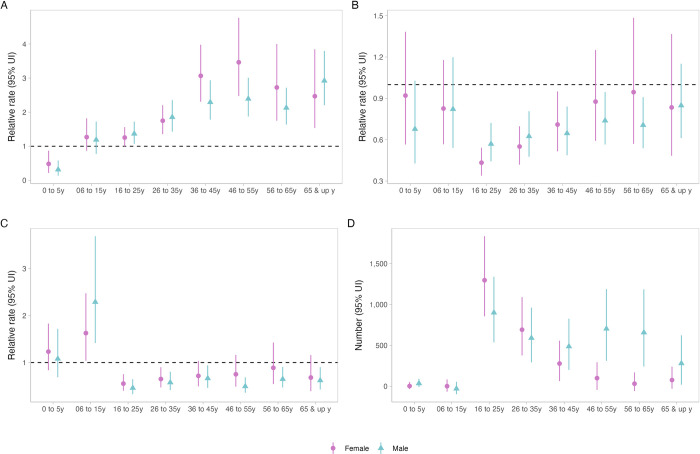
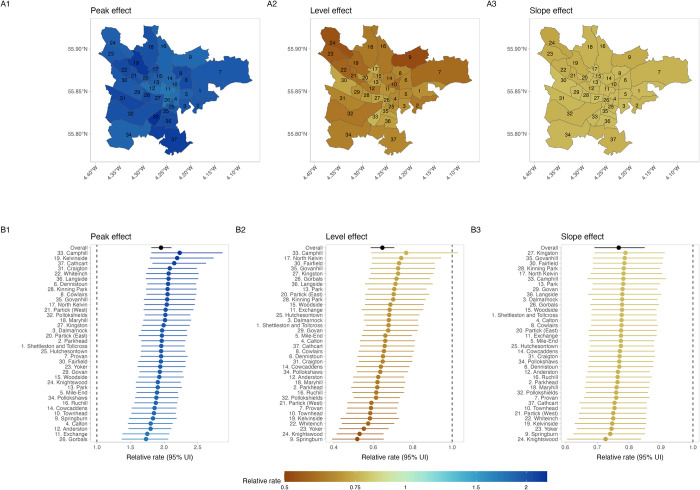
Case notifications for 1950 to 1963 were extracted from public health records and linked to demographic data. We fitted Bayesian multilevel regression models to estimate annual relative case notification rates (CNRs) during and after a mass screening intervention implemented over 5 weeks in 1957 compared to the counterfactual scenario where the intervention had not occurred. We additionally estimated case detection ratios and incidence. From 11 March 1957 to 12 April 1957, 714,915 people (622,349 of 819,301 [76.0%] resident adults ≥15 years) were screened with miniature chest X-ray; 2,369 (0.4%) were diagnosed with tuberculosis. Pre-intervention (1950 to 1956), pulmonary CNRs were declining at 2.3% per year from a CNR of 222/100,000 in 1950. With the intervention in 1957, there was a doubling in the pulmonary CNR (RR: 1.95, 95% uncertainty interval [UI] [1.81, 2.11]) and 35% decline in the year after (RR: 0.65, 95% UI [0.59, 0.71]). Post-intervention (1958 to 1963) annual rates of decline (5.4% per year) were greater (RR: 0.77, 95% UI [0.69, 0.85]), and there were an estimated 4,599 (95% UI [3,641, 5,683]) pulmonary case notifications averted due to the intervention. Effects were consistent across all city wards and notifications declined in young children (0 to 5 years) with the intervention. Limitations include the lack of data in historical reports on microbiological testing for tuberculosis, and uncertainty in contributory effects of other contemporaneous interventions including slum clearances, introduction of BCG vaccination programmes, and the ending of postwar food rationing.
A single, rapid round of mass screening with chest X-ray (probably the largest ever conducted) likely resulted in a major and sustained reduction in tuberculosis case notifications. Synthesis of evidence from other historical tuberculosis screening programmes is needed to confirm findings from Glasgow and to provide insights into ongoing efforts to successfully implement ACF interventions in today's high tuberculosis burden countries and with new screening tools and technologies.
1940 年至 1970 年间,社区活动性结核病病例发现(ACF)在欧洲和北美得到广泛实施,当时的发病率与许多当今高负担国家相当。我们采用中断时间序列分析,分析了 1957 年格拉斯哥大规模胸部 X 光检查活动对当代筛查方法的影响。
从公共卫生记录中提取了 1950 年至 1963 年的病例报告,并将其与人口统计数据相关联。我们拟合了贝叶斯多层次回归模型,以估计在 1957 年实施的为期 5 周的大规模筛查干预期间和之后的年度相对病例报告率(CNR),并与未发生干预的情况下的反事实情况进行了比较。我们还估计了病例检出率和发病率。从 1957 年 3 月 11 日至 4 月 12 日,对 714915 人(819301 名居民中≥15 岁的成年人[76.0%])进行了微型胸部 X 光检查;2369 人(0.4%)被诊断患有结核病。在干预前(1950 年至 1956 年),每年肺 CNR 下降 2.3%,1950 年 CNR 为 222/100000。1957 年的干预措施使肺 CNR 增加了一倍(RR:1.95,95%置信区间[1.81,2.11]),第二年下降了 35%(RR:0.65,95%置信区间[0.59,0.71])。干预后(1958 年至 1963 年),每年下降率(5.4%)更高(RR:0.77,95%置信区间[0.69,0.85]),估计由于干预措施,可避免 4599 例(95%置信区间[3641,5683])肺部病例报告。结果在所有城市行政区都一致,并且在干预后,幼儿(0 至 5 岁)的结核病病例也有所减少。局限性包括历史报告中缺乏结核病微生物学检测数据,以及不确定同期其他干预措施(包括贫民窟清理、卡介苗疫苗接种计划的引入以及战后食品配给制度的结束)的促成作用。
单次快速大规模 X 光筛查(可能是有史以来规模最大的一次)可能导致结核病病例报告的大幅和持续减少。需要综合其他历史结核病筛查计划的证据,以证实格拉斯哥的发现,并为当今高结核病负担国家成功实施 ACF 干预措施以及使用新的筛查工具和技术提供见解。