Luo Shan, Li Xiaohong, Wang Yan, Fan Wei, Zhang Long, Quan Yi, Huang Wei
( 610041) Department of Obstetrics and Gynecology, West China Second University Hospital, Sichuan University, Chengdu 610041, China.
() ( 610041) Key Laboratory of Birth Defects and Related Diseases of Women and Children of the Ministry of Education, Sichuan University, Chengdu 610041, China.
Sichuan Da Xue Xue Bao Yi Xue Ban. 2024 Sep 20;55(5):1288-1294. doi: 10.12182/20240960208.
To investigate effect of preimplantation genetic testing for aneuploidies (PGT-A) on the reproductive outcomes of women of advanced maternal age (AMA) (≥38 years), and to analyze factors influencing the live birth rate in AMA women who have received PGT-A.
A retrospective cohort study was conducted. AMA women undergoing PGT-A were enrolled in the PGT-A group. All of them underwent their first oocyte retrieval cycle between January 2019 and June 2023. AMA women undergoing fertilization/intracytoplasmic sperm injection (IVF/ICSI) and their first oocyte retrieval cycle over the same period of time were enrolled in the control group (the non-PGT-A group) via propensity score matching. The PGT-A group and the non-PGT-A group each included 193 cycles, which were followed up until January 2024. Follow-up concerning live births was completed for all oocyte retrieval cycles conducted between January 2019 and October 2022. The reproductive outcomes were compared between the two groups. The primary outcome indicator was cumulative live birth rate (CLBR) per oocyte retrieval, while the secondary outcome indicators were cumulative clinical pregnancy rate (CCPR) per oocyte retrieval and spontaneous abortion rate. For the 145 cycles in the PGT-A group with completed live birth follow-up, binary logistic regression analysis and receiver operator characteristic (ROC) curves were used to analyze the influencing factors of live birth rates.
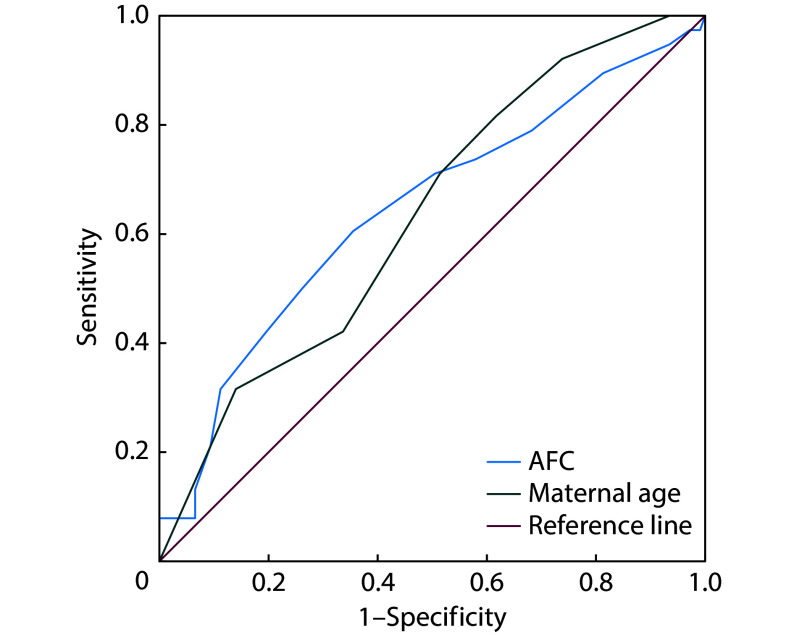
A total of 145 cycles in the PGT-A group and 161 cycles in the non-PGT-A group completed follow-up for live births. The CLBR per oocyte retrieval of the PGT-A group was 25.52% (37/145), while that of the non-PGT-A group was 28.50% (46/161), with no significant difference being observed between the two groups (<0.05). Of the 193 oocyte retrieval cycles in each group, 53 cycles in the PGT-A group and 72 cycles in the non-PGT-A group resulted in clinical pregnancies, with the difference in the CCPR per oocyte retrieval being statistically significant (27.46% vs. 37.31%, <0.05). Concerning clinical pregnancies, the spontaneous abortion rate of the PGT-A group was lower than that of the non-PGT-A group, with the difference being statistically significant (7.55% vs. 25.00%, <0.05). In AMA women who had undergone PGT-A for reproductive assistance, maternal age (odds ratio [OR]=0.786, 95% confidence interval [CI]: 0.635-0.973) and the antral follicle count (AFC) (OR=1.110, 95% CI: 1.013-1.216) were correlated with the outcome of live births outcome. The probability of live births decreased with increasing maternal age and decreasing AFC. When the female age was ≥42 years or when AFC≤8, the expected live birth outcome of PGT-A assisted pregnancy was poor.
PGT-A does not affect the CLBR per oocyte retrieval in AMA women, but it can effectively reduce the risks of implantation failure and spontaneous abortion due to fetal aneuploidies. For PGT-A-assisted pregnancy in AMA women, maternal age and AFC are important factors affecting the live birth outcomes.
探讨胚胎植入前非整倍体遗传学检测(PGT-A)对高龄产妇(≥38岁)生殖结局的影响,并分析影响接受PGT-A的高龄产妇活产率的因素。
进行一项回顾性队列研究。接受PGT-A的高龄产妇纳入PGT-A组。她们均在2019年1月至2023年6月期间进行首次取卵周期。通过倾向得分匹配,将同期接受体外受精/卵胞浆内单精子注射(IVF/ICSI)及首次取卵周期的高龄产妇纳入对照组(非PGT-A组)。PGT-A组和非PGT-A组各包含193个周期,随访至2024年1月。对2019年1月至2022年10月期间进行的所有取卵周期完成活产随访。比较两组的生殖结局。主要结局指标为每次取卵的累积活产率(CLBR),次要结局指标为每次取卵的累积临床妊娠率(CCPR)和自然流产率。对PGT-A组中145个完成活产随访的周期,采用二元逻辑回归分析和受试者工作特征(ROC)曲线分析活产率的影响因素。
PGT-A组共145个周期、非PGT-A组共161个周期完成活产随访。PGT-A组每次取卵的CLBR为25.52%(37/145),非PGT-A组为28.50%(46/161),两组间差异无统计学意义(<0.05)。每组193个取卵周期中,PGT-A组53个周期、非PGT-A组72个周期临床妊娠,每次取卵的CCPR差异有统计学意义(27.46%对37.31%,<0.05)。关于临床妊娠,PGT-A组的自然流产率低于非PGT-A组,差异有统计学意义(7.55%对25.00%,<0.05)。在接受PGT-A生殖辅助的高龄产妇中,产妇年龄(比值比[OR]=0.786,95%置信区间[CI]:0.635 - 0.973)和窦卵泡计数(AFC)(OR=1.110,95%CI:1.013 - 1.216)与活产结局相关。活产概率随产妇年龄增加和AFC降低而降低。当女性年龄≥42岁或AFC≤8时,PGT-A辅助妊娠的预期活产结局较差。
PGT-A不影响高龄产妇每次取卵的CLBR,但可有效降低因胎儿非整倍体导致的着床失败和自然流产风险。对于高龄产妇的PGT-A辅助妊娠,产妇年龄和AFC是影响活产结局的重要因素。