Ginsburg Liane, Easterbrook Adam, Geerts Ariane, Berta Whitney, van Dreumel Lynda, Estabrooks Carole A, Norton Peter G, Wagg Adrian
Health Policy and Management, York University Faculty of Health, Toronto, Ontario, Canada
The University of British Columbia-Vancouver Campus, Vancouver, British Columbia, Canada.
BMJ Qual Saf. 2025 Feb 19;34(3):146-156. doi: 10.1136/bmjqs-2024-017795.
There is growing recognition in the literature of the 'Herculean' efforts required to bring about change in healthcare processes and systems. Leadership is recognised as a critical lever for implementation of quality improvement (QI) and other complex team-level interventions; however, the processes by which leaders facilitate change are not well understood. The aim of this study is to examine 'how' leadership influences implementation of QI interventions.
We drew on the leadership literature and used secondary data collected as part of a process evaluation of the Safer Care for Older Persons in residential Environments (SCOPE) QI intervention to gain insights regarding the processes by which leadership influences QI implementation. Specifically, using detailed process evaluation data from 31 unit-based nursing home teams we conducted a thematic analysis with a codebook developed a priori based on the existing literature to identify leadership processes.
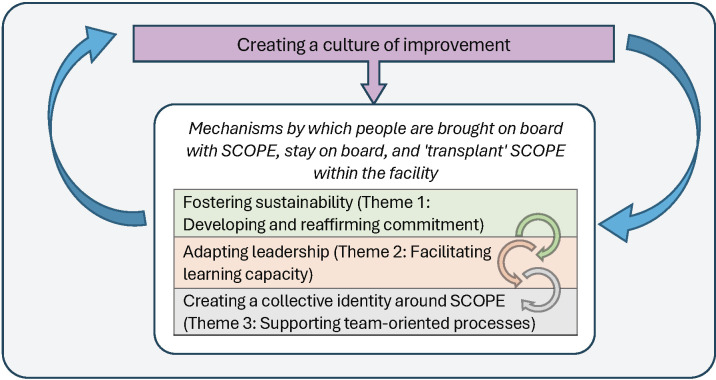
Effective leaders (ie, those who care teams felt supported by and who facilitated SCOPE implementation) successfully developed and reaffirmed teams' commitment to the SCOPE QI intervention (theme 1), facilitated learning capacity by fostering follower participation in SCOPE and empowering care aides to step into team leadership roles (theme 2) and actively supported team-oriented processes where they developed and nurtured relationships with their followers and supported them as they navigated relationships with other staff (theme 3). Together, these were the mechanisms by which care aides were brought on board with the intervention, stayed on board and, ultimately, transplanted the intervention into the facility. Building learning capacity and creating a culture of improvement are thought to be the overarching processes by which leadership facilitates implementation of complex interventions like SCOPE.
Results highlight important, often overlooked, relational and sociocultural aspects of successful QI leadership in nursing homes that can guide the design, implementation and scaling of complex interventions and can guide future research.
文献中越来越认识到,要在医疗保健流程和系统中实现变革需要付出“艰巨”努力。领导力被认为是实施质量改进(QI)和其他复杂团队层面干预措施的关键杠杆;然而,领导者促进变革的过程尚未得到充分理解。本研究的目的是探讨领导力如何影响QI干预措施的实施。
我们借鉴了领导力文献,并使用作为“住宅环境中老年人更安全护理”(SCOPE)QI干预措施过程评估的一部分收集的二手数据,以深入了解领导力影响QI实施的过程。具体而言,我们使用来自31个基于单元的养老院团队的详细过程评估数据,基于现有文献预先制定了编码手册,进行了主题分析,以确定领导过程。
有效的领导者(即那些护理团队感到得到支持并促进SCOPE实施的领导者)成功地培养并重申了团队对SCOPE QI干预措施的承诺(主题1),通过促进追随者参与SCOPE并赋予护理助手担任团队领导角色的权力来促进学习能力(主题2),并积极支持以团队为导向的过程,在这些过程中,他们与追随者建立并培养关系,并在追随者与其他工作人员建立关系时给予支持(主题3)。这些共同构成了护理助手参与干预措施、持续参与并最终将干预措施引入机构的机制。建立学习能力和营造改进文化被认为是领导力促进像SCOPE这样的复杂干预措施实施的总体过程。
研究结果突出了养老院成功实施QI领导力中重要但往往被忽视的关系和社会文化方面,这些方面可以指导复杂干预措施的设计、实施和推广,并可为未来研究提供指导。