Kiritsi Dimitra, Schauer Franziska, Gewert Stella, Reineker Katja, Reimer-Taschenbrecker Antonia, Schwieger-Briel Agnes, Ott Hagen, Schmoor Claudia, Grishina Olga, Murrell Dedee, Stiller Brigitte, Zahn Tobias, Nyström Alexander, Bruckner-Tuderman Leena
Department of Dermatology, Medical Center- University of Freiburg, Faculty of Medicine, University of Freiburg, Freiburg, Germany.
First Department of Dermatology, Faculty of Medicine, Aristotle University of Thessaloniki, Thessaloniki, Greece.
EClinicalMedicine. 2024 Oct 30;77:102900. doi: 10.1016/j.eclinm.2024.102900. eCollection 2024 Nov.
Recessive dystrophic epidermolysis bullosa (RDEB) is a skin fragility disorder characterised by life-long mechanically induced skin blistering, fibrosis-driven pseudosyndactyly, and multi-organ involvement. Preclinical studies have suggested mitigated progression by angiotensin II type I receptor blockade through losartan. We aimed to determine the safety and tolerability of systemic losartan treatment among children with RDEB, and to obtain initial data on its clinical benefit.
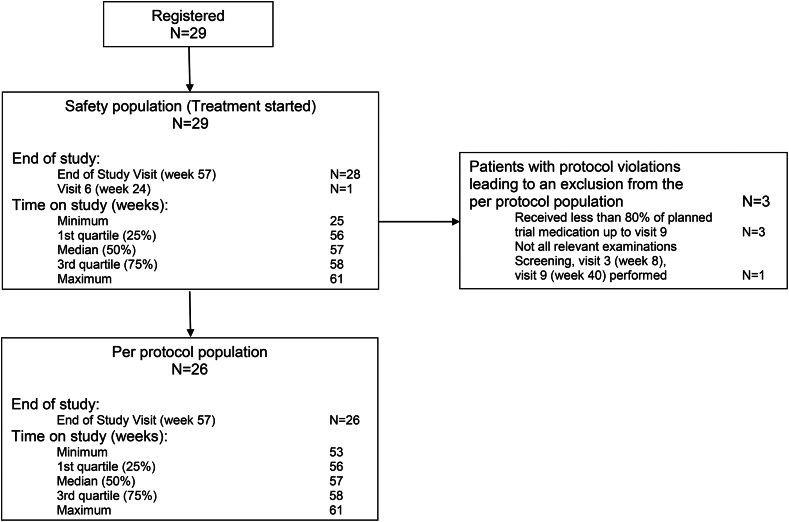
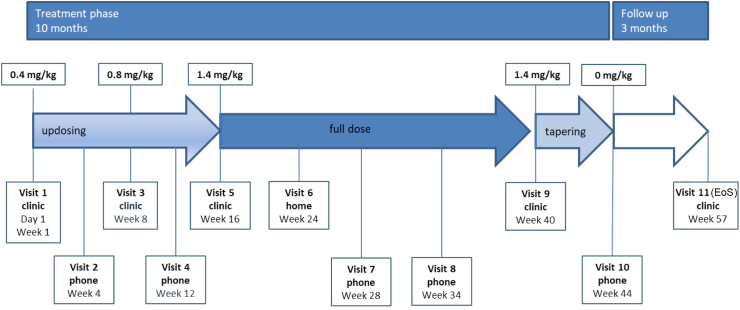
We conducted an open-label, single-arm, phase 1/2 trial at the Medical Center-University of Freiburg, Germany. Children with molecularly-confirmed RDEB, aged 2-16 years (starting from the 25th month of life) were eligible. Key exclusion criteria comprised anaemia with haemoglobin <8 g/dl; hypotension (defined as age-related systolic blood pressure under the 5th percentile); cardiologic contraindications, requirement for any medications that are likely to cause interactions with losartan; renal artery stenosis or renal insufficiency with creatinine clearance <30 ml/min; severe liver failure; severe, untreated electrolyte disturbances; history of cancer or chronic viral infections; hypersensitivity to losartan or any of the excipients and known or persistent abuse of medication, drugs, or alcohol. Treatment duration with losartan comprised 10 months, encompassing 16 weeks up-dosing of losartan, 24 weeks full dose losartan (final target dose of 1.4 mg/kg), and 4 weeks losartan tapering, followed by 12 weeks follow-up without losartan. The primary endpoint was occurrence of a serious safety concern, defined as one of the following side effects of losartan: clinically relevant severe hypotension, immediate hypersensitivity reactions to the drug or clinical relevant severe hypo- and hyperkalaemia. EB-specific scores (the EBDASI activity and damage score, Birmingham Epidermolysis Bullosa Severity Score (BEBS)) and other clinical outcome parameters were evaluated at five clinical visits as secondary outcomes: pain (Wong-Baker FACES Scale for pain), quality of life (Quality Of Life in EB [QOLEB] questionnaire and Children's Dermatology Life Quality Index [CDLQI]), itch (Itch Assessment Scale for the Paediatric Burn Patients), dysphagia (Mayo Dysphagia Questionnaire-day 30 [MDQ-30]), pseudosyndactyly progression (our own morphometric scoring instrument), and hand function (Score of Colville and Terrill). All analyses (safety and efficacy) were performed in the safety population, defined as participants who received at least one dose of trial medication with losartan. This trial is registered with EudraCT, 2015-003670-32.
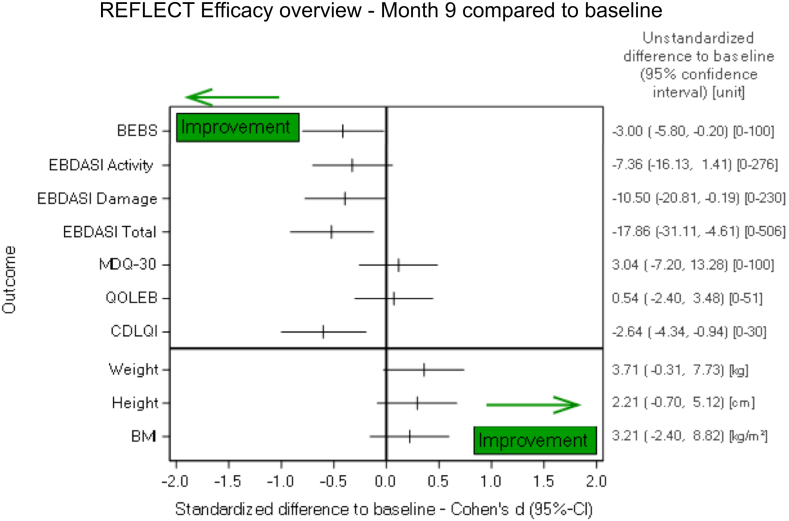
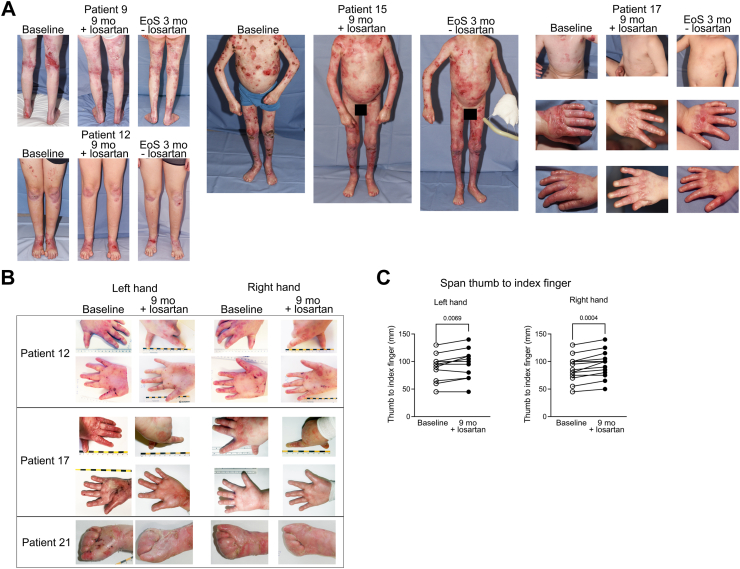
Between Jul 28, 2017, and Feb 12, 2021, 29 children were enrolled. Of those 27 received the full treatment. Losartan was well tolerated, no treatment-related severe complications leading to a serious safety concern occurred. The patients revealed improvement in the RDEB clinical scores, namely a mean reduction at week 40 of -7.36 points (95%-CI: -16.13 to 1.41) in the EBDASI activity score and -10.50 points (95%-CI: -20.81 to -0.19) in the EBDASI damage score, while the Children's Dermatology Life Quality Index rose by 2.64 points (95%-CI: -4.55 to -0.90). Similar to the EBDASI score, the BEBS showed a mean reduction of -3 points, 95%-CI: -0.21 to -5,79, P = 0.036). In the Wong-Baker FACES Scale for Pain an improvement of at least one level was identified for 9 of 28 patients between baseline and at month 9 (95%-CI: 15.9%-52.4%; P = 0.57). Regarding the Quality of Life in EB Score, five of 28 patients showed an improvement in the total scale of at least one level at month 9 (95%-CI: 6.1%-36.9%; P = 0.71). With the Itch assessment scale for the paediatric burn patients an improvement of at least one level could be observed in 12 of 28 patients (95%-CI: 24.5%-62.8%; P = 0.24). The MDQ-30 showed no relevant difference at 9 months after treatment start, as compared to baseline. We observed improvement of finger span with our own morphometric scoring instrument of pseudosyndactyly progression, revealing an increase of the maximal distance between thumb and index finger at month 9 by 6.92 mm, 95%-CI [3.48, 10.37] P = 0.0009. With the Hand function assessment score of Colville and Terrill, an improvement of at least one level was documented for 3 of 28 patients, i.e., 10.7% (95%-CI: 2.3%-28.2%; P = 0.63).
Our results suggest that losartan was well tolerated by children with RDEB, and provide preliminary evidence that it may reduce disease burden. Further research with larger sample sizes and longer durations is needed to establish the treatment's long-term efficacy and safety.
Debra International, the Department of Dermatology, Medical Center-University of Freiburg (Berta-Ottenstein Advanced Clinician Scientist Program of the Medical Faculty), and the German Research Foundation.
隐性营养不良性大疱性表皮松解症(RDEB)是一种皮肤脆性疾病,其特征为终生因机械作用导致皮肤水疱形成、纤维化驱动的假性并指以及多器官受累。临床前研究表明,通过氯沙坦阻断血管紧张素II 1型受体可减缓疾病进展。我们旨在确定氯沙坦全身治疗在RDEB患儿中的安全性和耐受性,并获取其临床获益的初步数据。
我们在德国弗莱堡大学医学中心进行了一项开放标签、单臂、1/2期试验。年龄在2至16岁(从出生后第25个月起)且分子确诊为RDEB的儿童符合条件。主要排除标准包括:血红蛋白<8 g/dl的贫血;低血压(定义为年龄相关的收缩压低于第5百分位数);心脏疾病禁忌证;需要使用任何可能与氯沙坦发生相互作用的药物;肾动脉狭窄或肌酐清除率<30 ml/min的肾功能不全;严重肝功能衰竭;严重的、未经治疗的电解质紊乱;癌症或慢性病毒感染史;对氯沙坦或任何辅料过敏以及已知或持续滥用药物、毒品或酒精。氯沙坦的治疗持续时间为10个月,包括16周的氯沙坦剂量递增期、24周的氯沙坦全剂量期(最终目标剂量为1.4 mg/kg)以及4周的氯沙坦减量期。之后为12周的无氯沙坦随访期。主要终点是出现严重安全问题,定义为氯沙坦的以下副作用之一:临床相关的严重低血压、对药物的即刻过敏反应或临床相关的严重低钾血症和高钾血症。在五次临床访视时评估EB特异性评分(EBDASI活动和损伤评分、伯明翰大疱性表皮松解症严重程度评分(BEBS))以及其他临床结局参数作为次要结局:疼痛(采用Wong-Baker面部表情疼痛量表)、生活质量(采用EB生活质量[QOLEB]问卷和儿童皮肤病生活质量指数[CDLQI])、瘙痒(采用小儿烧伤患者瘙痒评估量表)、吞咽困难(采用梅奥吞咽问卷-第30天[MDQ-30])、假性并指进展(我们自己的形态计量评分工具)以及手部功能(科尔维尔和特里尔评分)。所有分析(安全性和有效性)均在安全人群中进行,安全人群定义为接受至少一剂含氯沙坦试验药物的参与者。本试验已在欧洲临床试验数据库(EudraCT)注册,注册号为2015-003670-32。
在2017年7月28日至2021年2月12日期间,共纳入29名儿童。其中27名接受了全程治疗。氯沙坦耐受性良好,未发生导致严重安全问题的与治疗相关的严重并发症。患者的RDEB临床评分有所改善,具体如下:在第40周时,EBDASI活动评分平均降低-7.36分(95%置信区间:-16.13至1.41),EBDASI损伤评分平均降低-10.50分(95%置信区间:-20.81至-0.19),而儿童皮肤病生活质量指数上升了2.64分(95%置信区间:-4.55至-0.90)。与EBDASI评分类似,BEBS平均降低-3分,95%置信区间:-0.21至-5.79,P = 0.036)。在Wong-Baker面部表情疼痛量表中,28名患者中有9名在基线至第9个月期间疼痛至少改善了一个等级(95%置信区间:15.9%-52.4%;P = 0.57)。关于EB生活质量评分,28名患者中有5名在第9个月时总评分至少改善了一个等级(95%置信区间:6.1%-36.9%;P = 0.71)。在小儿烧伤患者瘙痒评估量表中,28名患者中有12名至少改善了一个等级(95%置信区间:24.5%-62.8%;P = 0.24)。治疗开始后9个月时,MDQ-30与基线相比无显著差异。我们使用自己的假性并指进展形态计量评分工具观察到指间距有所改善,在第9个月时拇指与食指之间的最大距离增加了6.92 mm,95%置信区间为[3.48, 10.37],P = 0.0009。在科尔维尔和特里尔的手部功能评估评分中,28名患者中有3名记录到至少改善了一个等级,即10.7%(95%置信区间:2.3%-28.2%;P = 0.63)。
我们的结果表明,RDEB患儿对氯沙坦耐受性良好,并提供了初步证据表明其可能减轻疾病负担。需要进行更大样本量和更长疗程的进一步研究,以确定该治疗方法的长期疗效和安全性。
德布拉国际、弗莱堡大学医学中心皮肤科(医学院的贝塔 - 奥滕斯坦高级临床科学家项目)以及德国研究基金会。