Pu Jiaxi, Gao Ming, Yu Pan, Tian Jiaqi, Yan Junxia, Yuan Qiongjing, Tao Lijian, Peng Zhangzhe
Department of Nephrology, Xiangya Hospital, Central South University, Changsha, 410008, China.
Department of Geriatric Medicine, Center of Coronary Circulation, Xiangya Hospital, Central South University, Changsha, 410008, China.
Diabetol Metab Syndr. 2024 Nov 14;16(1):272. doi: 10.1186/s13098-024-01514-6.
Type 2 diabetes mellitus (T2DM) poses a substantial global health concern. Statins are widely used among T2DM patients for managing dyslipidemia, preventing cardiovascular disease (CVD), and offering renal protection. However, the extent to which their renal protective effects contribute to reducing the incidence of severe renal complications, including chronic kidney disease (CKD) and renal failure, is not well-defined.
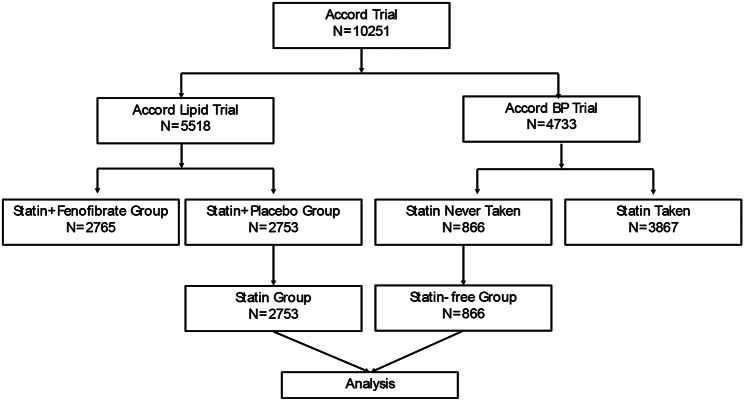
This investigation scrutinizes the impact of simvastatin versus placebo on renal outcomes among T2DM patients utilizing data from the ACCORD trial. It encompasses incidence rate comparisons, Kaplan-Meier estimates, Cox proportional hazards models, and mediation analyses.
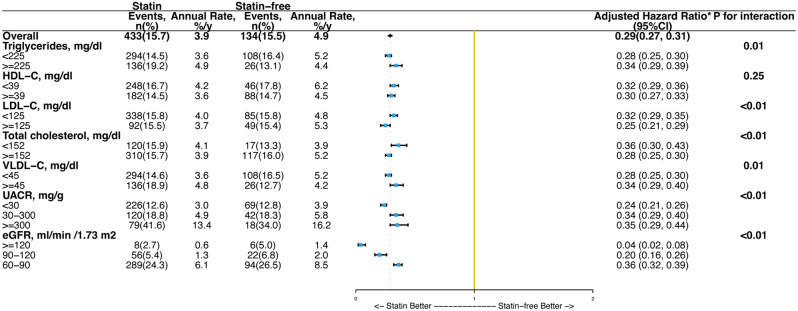
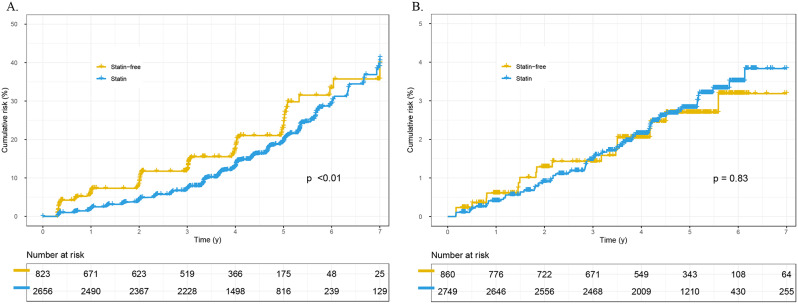
The study consisted of 3,619 individuals diagnosed with T2DM, among which 2,753 were treated routinely with simvastatin, while 866 did not receive any statin therapy. After adjusting for baseline characteristics and time-dependent covariates, simvastatin treatment was associated with a 71% reduction in the risk of CKD (HR 0.29, 95% CI 0.27-0.31, p < 0.01) and a 47% reduction in the risk of renal failure (HR 0.53, 95% CI 0.44-0.65, p < 0.01) compared to the statin-free group. Further subgroup analysis, accounting for the initial lipid and kidney profiles, indicated variable impacts of simvastatin on CKD and renal failure outcomes. Nevertheless, a consistent reduction in CKD risk was observed across all subgroups within the statin-treated population. Additional mediation analysis revealed that the reduction in low-density lipoprotein cholesterol (LDL-C) may be a potential mediator in the association between simvastatin and CKD, with a mediation effect of 14.9%, (95% CI 0.11-0.19, p < 0.01).
Administering statins, specifically simvastatin, to T2DM patients at elevated risk for CVD, is likely to offer augmented renal advantages, notably in lowering the occurrence of CKD and renal failure. This protective effect against CKD manifests regardless of initial lipid profiles, albuminuria, and estimated glomerular filtration rate (eGFR) levels. The association between simvastatin and CKD may be partially mediated by LDL-C reduction.
2型糖尿病(T2DM)是一个重大的全球健康问题。他汀类药物在T2DM患者中广泛用于管理血脂异常、预防心血管疾病(CVD)以及提供肾脏保护。然而,其肾脏保护作用在降低包括慢性肾脏病(CKD)和肾衰竭在内的严重肾脏并发症发生率方面的贡献程度尚不明确。
本研究利用ACCORD试验的数据,仔细研究了辛伐他汀与安慰剂对T2DM患者肾脏结局的影响。包括发病率比较、Kaplan-Meier估计、Cox比例风险模型和中介分析。
该研究纳入了3619例诊断为T2DM的个体,其中2753例常规接受辛伐他汀治疗,866例未接受任何他汀类药物治疗。在调整基线特征和时间依赖性协变量后,与未使用他汀类药物的组相比,辛伐他汀治疗使CKD风险降低71%(HR 0.29,95%CI 0.27 - 0.31,p < 0.01),肾衰竭风险降低47%(HR 0.53,95%CI 0.44 - 0.65,p < 0.01)。进一步的亚组分析,考虑到初始血脂和肾脏状况表明,辛伐他汀对CKD和肾衰竭结局有不同影响。然而,在接受他汀类药物治疗的人群中,所有亚组的CKD风险均持续降低。额外的中介分析显示,低密度脂蛋白胆固醇(LDL-C)的降低可能是辛伐他汀与CKD关联中的一个潜在中介因素,中介效应为14.9%,(95%CI 0.11 - 0.19,p < 0.01)。
对心血管疾病风险较高的T2DM患者使用他汀类药物,特别是辛伐他汀,可能会带来更大的肾脏益处,尤其是在降低CKD和肾衰竭的发生率方面。这种对CKD的保护作用无论初始血脂状况、蛋白尿和估计肾小球滤过率(eGFR)水平如何都会显现。辛伐他汀与CKD之间的关联可能部分由LDL-C的降低介导。