Izumi Rina, Hayashi Koji, Nakaya Yuka, Suzuki Asuka, Takaku Naoko, Sato Mamiko, Kobayashi Yasutaka
Department of Rehabilitation Medicine, Fukui General Hospital, Fukui, JPN.
Graduate School of Health Science, Fukui Health Science University, Fukui, JPN.
Cureus. 2024 Oct 19;16(10):e71880. doi: 10.7759/cureus.71880. eCollection 2024 Oct.
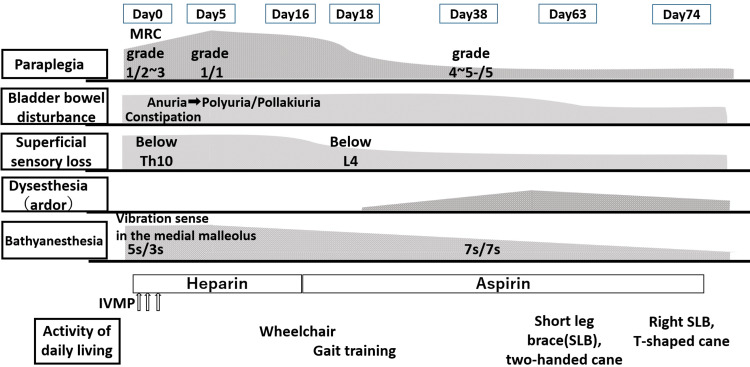
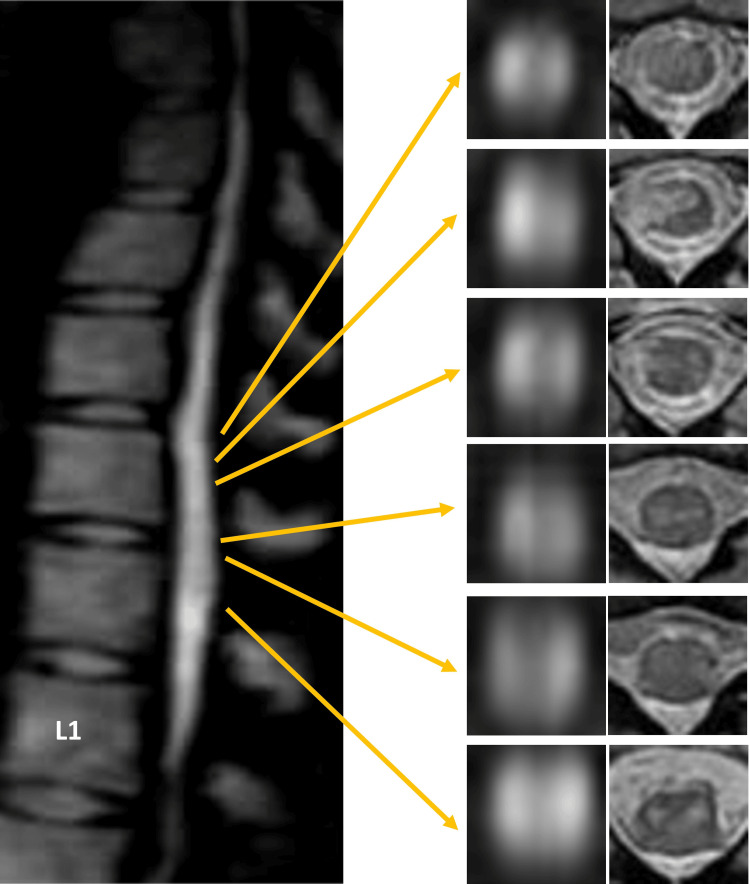
Spinal cord infarction (SCI) is a rare vascular condition that can lead to the sudden onset of myelopathy, manifesting as paraplegia, bladder and bowel dysfunction, and/or sensory impairments. The primary arteries supplying the spinal cord are the anterior spinal artery (ASA) and the posterior spinal artery (PSA). The ASA mainly provides blood to the anterior two-thirds of the spinal cord, excluding the posterior columns, while the PSA primarily supplies the posterior one-third, which includes the posterior columns. It is relatively uncommon for vascular SCI to result in complete sensory loss, as the area supplied by the ASA is mainly associated with superficial sensation, while the PSA is related to deep sensation. In this report, we describe a case of SCI with pansensory deficits and explore the potential causes of pansensory loss in SCI. The patient was a 51-year-old healthy woman who experienced sudden lower back discomfort, progressing to bilateral lower limb weakness within 30 minutes, accompanied by urinary retention after lifting a heavy object. She was transferred to the hospital with stable vitals except for high blood pressure. A neurological examination revealed significant weakness in her lower limbs, hypesthesia below the Th10 level, bathyanesthesia, and areflexia. Spinal MRI showed hyperintensities at the Th11-Th12 levels, leading to a diagnosis of spinal cord infarction. She was treated with methylprednisolone, heparin, and rehabilitation. Over time, her muscle strength and sensory loss improved, though dysesthesia persisted. After 80 days of treatment and rehabilitation, she was able to walk independently with assistance and was discharged.
脊髓梗死(SCI)是一种罕见的血管疾病,可导致脊髓病突然发作,表现为截瘫、膀胱和肠道功能障碍及/或感觉障碍。供应脊髓的主要动脉是脊髓前动脉(ASA)和脊髓后动脉(PSA)。ASA主要为脊髓前三分之二供血,不包括后柱,而PSA主要供应后三分之一,包括后柱。血管性SCI导致完全性感觉丧失相对少见,因为ASA供血区域主要与浅感觉相关,而PSA与深感觉相关。在本报告中,我们描述了一例伴有全感觉缺失的SCI病例,并探讨了SCI中全感觉丧失的潜在原因。患者为一名51岁健康女性,突然出现下背部不适,30分钟内进展为双下肢无力,重物搬运后伴有尿潴留。除高血压外,生命体征稳定,被转至医院。神经系统检查显示双下肢明显无力,T10水平以下感觉减退、深感觉障碍及反射消失。脊髓MRI显示T11 - T12水平高信号,诊断为脊髓梗死。给予甲泼尼龙、肝素治疗及康复治疗。随着时间推移,她的肌肉力量和感觉丧失有所改善,但感觉异常持续存在。经过80天的治疗和康复,她能够在辅助下独立行走并出院。