Hora Rhythm, Ray Arindam, Longchar Imkongtemsu, Rio G R, Mehra Rashmi, Koshal Seema Singh, Kumari Amrita, Quadri Syed F, Kaur Amanjot, Roy Arup Deb
John Snow India, New Delhi, India.
Bill and Melinda Gates Foundation, New Delhi, India.
Vaccine X. 2024 Nov 1;21:100578. doi: 10.1016/j.jvacx.2024.100578. eCollection 2024 Dec.
Worldwide, vaccine-preventable diseases have been a significant cause of mortality in the under-5 age group. To reduce the disease burden, new vaccines are being introduced in every country's immunization programmes. For this to happen, high vaccination coverage is necessary. However, rapidly identifying the areas that fail to reach the expected coverage becomes cumbersome. During recent years, lot quality assurance sampling (LQAS) has been widely used in evaluating immunization coverage across the globe. The present study aims to pilot this approach for field monitoring of a new vaccine against routine concurrent field monitoring in one of the North-Eastern states of India.
For LQAS, a community-based cross-sectional study was undertaken among 55 children aged 0-23 months in all 5 Primary health centres (lots) of Medziphema block, Dimapur, Nagaland. The total sample size for LQAS was calculated based on α = 5, β = 90 using Lemeshow and Taber-LQAS table with a target level of immunization defined as 90 % and the lower limit set to 55 %. For the concurrent field monitoring, a sample of 30 children in the same age group was selected through random sampling. Pre-designed, pre-tested questionnaire for the caregivers, scripted on a digital tool was employed with verification of immunization card and caregiver's recall. Data was analyzed using SPSS software version 25.0.
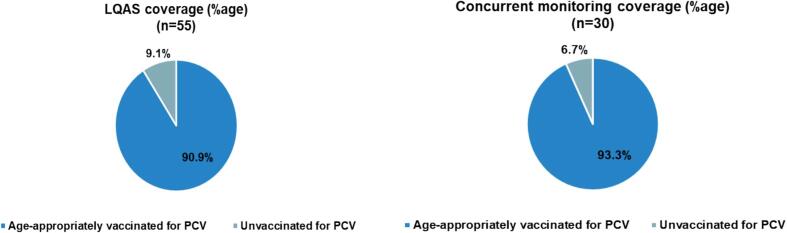
The study found a slight difference in the percentage of children age-appropriately vaccinated for PCV (as per the schedule) in concurrent field monitoring (93.3 %) and LQAS (90.9 %). However, no statistically significant difference was found in comparing the immunization coverage using both methodologies (p > 0.05).
The study findings encourage that LQAS can be considered for monitoring the immunization coverage of a newly introduced vaccine. It offers the added advantage of identifying poor/low-performing pockets that require focused attention.
在全球范围内,疫苗可预防疾病一直是5岁以下儿童死亡的重要原因。为减轻疾病负担,各国的免疫规划中都在引入新疫苗。要实现这一点,高疫苗接种覆盖率是必要的。然而,迅速找出未达到预期覆盖率的地区变得很麻烦。近年来,批量质量保证抽样(LQAS)已在全球广泛用于评估免疫接种覆盖率。本研究旨在试点这种方法,以对印度东北部某邦的一种新疫苗进行现场监测,并与常规现场监测进行对比。
对于LQAS,在那加兰邦迪马普尔县梅齐费马区的所有5个初级卫生中心(批次)中,对55名年龄在0至23个月的儿童进行了基于社区的横断面研究。LQAS的总样本量是根据α = 5、β = 90,使用Lemeshow和Taber-LQAS表计算得出的,免疫接种目标水平定义为90%,下限设定为55%。对于同步现场监测,通过随机抽样在同一年龄组中选取了30名儿童。使用预先设计、预先测试的针对看护人的问卷,该问卷记录在数字工具上,并核查免疫接种卡和看护人的回忆情况。使用SPSS 25.0软件进行数据分析。
研究发现,在同步现场监测(93.3%)和LQAS(90.9%)中,按计划年龄适当接种肺炎球菌结合疫苗(PCV)的儿童百分比略有差异。然而,在比较两种方法的免疫接种覆盖率时,未发现统计学上的显著差异(p > 0.05)。
研究结果表明,可以考虑使用LQAS来监测新引入疫苗的免疫接种覆盖率。它具有识别需要重点关注的较差/表现不佳区域的额外优势。