Department of Endocrinology, Morbid Obesity and Preventive Medicine, Oslo University Hospital, Oslo, Norway.
Institute of Clinical Medicine, Faculty of Medicine, University of Oslo, Oslo, Norway.
Cardiovasc Diabetol. 2024 Nov 19;23(1):419. doi: 10.1186/s12933-024-02509-3.
Individuals with type 1 diabetes are at increased risk of accelerated atherosclerosis, causing coronary artery disease (CAD). The underlying mechanisms remain unclear, but new theories proposed are damage of gut mucosa causing leakage and translocation of gut microbiota products into the circulation, leading to inflammatory responses and atherosclerosis. We therefore aimed to study the associations between gut related inflammatory biomarkers and coronary atherosclerosis in individuals with long-term type 1 diabetes.
In this cross-sectional, controlled study of 102 participants with type 1 diabetes and 63 control subjects, we measured circulating levels of intestinal fatty acid binding protein (I-FABP), soluble cluster of differentiation 14 (sCD14), lipopolysaccharide binding protein (LBP) and interleukin 18 (IL-18) by enzyme-linked immunosorbent assay (ELISA), and further gene expression of CD14 and toll-like receptor 4 (TLR4) by real time PCR in circulating leukocytes and peripheral blood mononuclear cells (PBMCs). The participants had either established coronary heart disease (CHD) or underwent computed tomography coronary angiography (CTCA) to assess for coronary atherosclerosis, including total, calcified and soft/mixed plaque volumes.
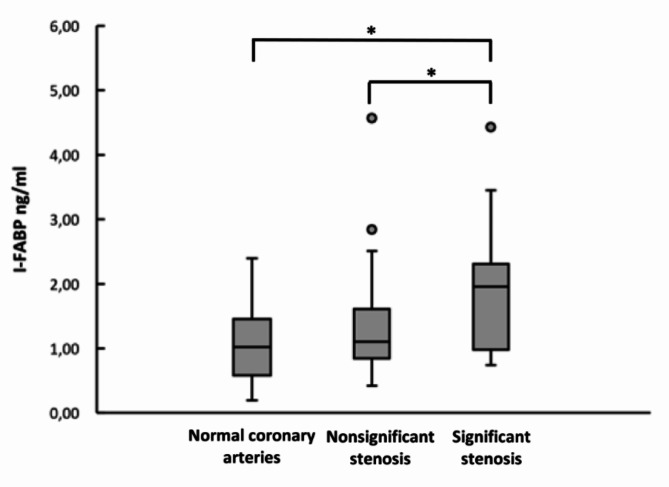
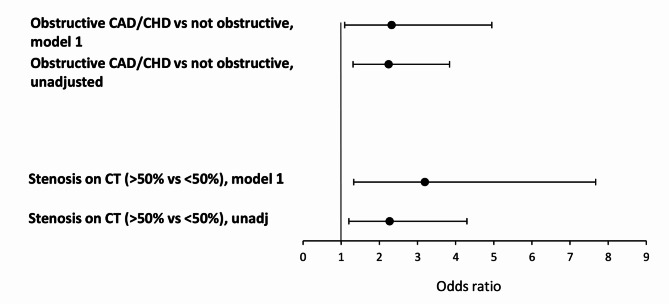
In the diabetes group, the levels of I-FABP were significantly higher in participants with established CHD or significant stenosis on CTCA compared to the participants with normal arteries or non-significant stenosis, with median 1.67 ng/ml (interquartile range [IQR] 1.02-2.32) vs. median 1.09 ng/ml (IQR 0.82-1.58), p = 0.003. I-FABP was associated with significant coronary artery stenosis by CTCA (> 50%) or previously established CHD in the adjusted analysis (odds ratio [OR] = 2.32, 95% confidence interval [CI]: 1.09-4.95; p = 0.029). The levels of I-FABP correlated also to total coronary plaque volume (r = 0.22, p < 0.05). This association remained significant after adjusting for age, sex, persistent albuminuria, eGFR, statin treatment, diabetes duration and mean time-weighted variables; HbA1c, LDL-cholesterol and systolic blood pressure (OR = 1.97, 95% CI: 1.28-3.01; p = 0.002).
In this cohort of individuals with long-term type 1 diabetes I-FABP associated significantly with coronary artery stenosis, suggesting a potential role of gut mucosa damage in the process of atherosclerosis in type 1 diabetes.
1 型糖尿病患者发生动脉粥样硬化加速的风险增加,导致冠状动脉疾病(CAD)。其潜在机制尚不清楚,但提出的新理论是肠道黏膜损伤导致肠道微生物产物渗漏和易位进入循环,引起炎症反应和动脉粥样硬化。因此,我们旨在研究长期 1 型糖尿病患者肠道相关炎症生物标志物与冠状动脉粥样硬化之间的关系。
在这项横断面、对照研究中,纳入了 102 名 1 型糖尿病患者和 63 名对照者,我们通过酶联免疫吸附试验(ELISA)测量了循环中肠脂肪酸结合蛋白(I-FABP)、可溶性 CD14(sCD14)、脂多糖结合蛋白(LBP)和白细胞介素 18(IL-18)的水平,并通过实时 PCR 进一步测量了循环白细胞和外周血单核细胞(PBMC)中 CD14 和 Toll 样受体 4(TLR4)的基因表达。参与者要么已经患有冠心病(CHD),要么接受计算机断层冠状动脉造影(CTCA)以评估冠状动脉粥样硬化,包括总斑块、钙化斑块和软/混合斑块体积。
在糖尿病组中,与动脉正常或狭窄不显著的参与者相比,已有 CHD 或 CTCA 显示有严重狭窄的参与者的 I-FABP 水平明显更高,中位数分别为 1.67ng/ml(四分位间距 [IQR] 1.02-2.32)和 1.09ng/ml(IQR 0.82-1.58),p=0.003。在调整分析中,I-FABP 与 CTCA 显示有显著冠状动脉狭窄(>50%)或之前已确诊的 CHD 相关(比值比 [OR] 2.32,95%置信区间 [CI]:1.09-4.95;p=0.029)。I-FABP 水平也与总冠状动脉斑块体积相关(r=0.22,p<0.05)。在调整年龄、性别、持续白蛋白尿、eGFR、他汀类药物治疗、糖尿病病程和平均时间加权变量;HbA1c、LDL-胆固醇和收缩压后,这种关联仍然显著(OR 1.97,95%CI:1.28-3.01;p=0.002)。
在这项长期 1 型糖尿病患者队列研究中,I-FABP 与冠状动脉狭窄显著相关,表明肠道黏膜损伤在 1 型糖尿病动脉粥样硬化过程中可能起作用。