Gastroenterology-Liver-Endoscopy Unit, 2nd Department of Internal Medicine, General Hospital of Athens "Hippocration", National and Kapodistrian University of Athens, Athens, Greece.
Department of Gastroenterology and Hepatology, Athens Medical - P. Faliron Hospital, Athens, Greece.
BMC Gastroenterol. 2024 Nov 21;24(1):420. doi: 10.1186/s12876-024-03483-6.
Patients with cirrhosis and portal hypertension may have alterations in intestinal barrier resulting in increased susceptibility for infections. We investigated the effect of propranolol in gastrointestinal motility, permeability and bacterial overgrowth in cirrhosis.
Patients with cirrhosis and esophageal varices were studied before and after a build-up dose of propranolol according to standard guidelines. Serum TNF-a, IL-6, IL-1b, LPS and bacterial DNA were measured before and during propranolol therapy. Oro-caecal transit time (OCTT) and bacterial overgrowth (BO) have been evaluated with H2 breath testing. Intestinal paracellular (IP), cellular passive non-carrier (ICNC), cellular passive carrier-mediated (ICCM), and gastric permeability (GP) were evaluated by measurement of lactulose, mannitol, D-xylose and sucrose respectively in urine, with high performance liquid chromatography (HPLC).
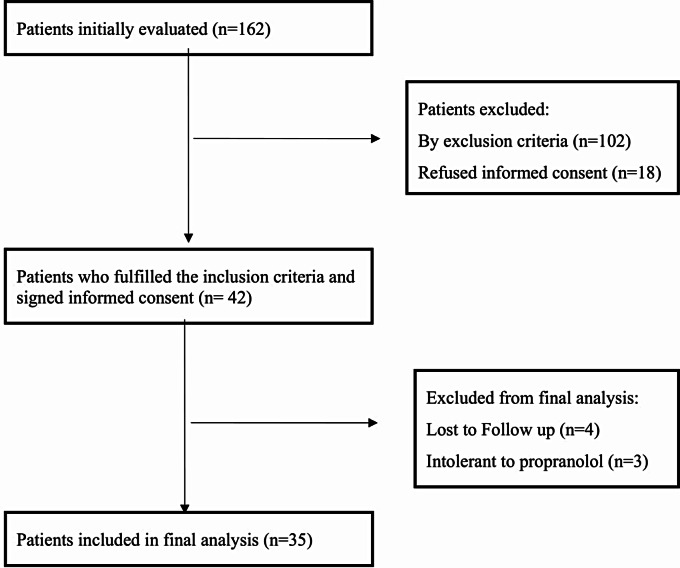
35 patients with cirrhosis and portal hypertension with median age was 59.6 years (range 42-86) were included in the study. Twenty one had viral hepatitis and 25 were classified as having advanced cirrhosis (Child-Pugh B: 14 or C: 11). Median dose of administrated propranolol was 40 mg/day. After 7 days propranolol treatment BO was resolved in 15 out of 16 patients (93.7%, p = 0.0001) and OCTT was reduced significantly from 180 min to 139 min (SD 58.5, difference - 4 1 min, p = 0.0001). Serum IL-6 levels were reduced in 21/35 (60%) patients from 41.1 to 19 pg/ml (p = 0.01), TNF-a in 10/35 (28.5%) patients from 10.7 to 5.6 pg/ml (p = 0.007) and LPS in 20/35 (57%) from 7.1 to 5.2 mg/L (p = 0.1). No bacterial DNA was detected in serum of all patients either baseline or under propranolol treatment. IP was significantly reduced (0.2 to 0.16, p = 0.04) whereas ICNC (p = 0.9), ICCM (p = 0.4) and GP (p = 0.7) were not affected significantly. Intestinal Permeability (PI) index (Lactulose to Mannitol ratio) was significantly reduced (0.027 to 0.02, p = 0.03).
In patients with cirrhosis and portal hypertension, propranolol use is associated with reduction in BO, increase in intestinal motility and amelioration in intestinal permeability. Moreover IL-6 and LPS levels are being decreased in the majority of patients under propranolol.
肝硬化和门静脉高压患者的肠道屏障可能会发生改变,从而导致更容易感染。我们研究了普萘洛尔对肝硬化患者胃肠动力、通透性和细菌过度生长的影响。
根据标准指南,对患有肝硬化和食管静脉曲张的患者在普萘洛尔增量剂量前后进行研究。在普萘洛尔治疗前后测量血清 TNF-a、IL-6、IL-1b、LPS 和细菌 DNA。通过 H2 呼气试验评估口盲肠转运时间(OCTT)和细菌过度生长(BO)。通过测量尿液中乳果糖、甘露醇、D-木糖和蔗糖,分别用高效液相色谱法(HPLC)评估肠细胞旁(IP)、细胞被动非载体(ICNC)、细胞被动载体介导(ICCM)和胃通透性(GP)。
本研究共纳入 35 例中位年龄为 59.6 岁(范围 42-86 岁)的肝硬化伴门静脉高压患者。21 例为病毒性肝炎,25 例为晚期肝硬化(Child-Pugh B:14 例或 C:11 例)。给予的普萘洛尔中位剂量为 40mg/天。普萘洛尔治疗 7 天后,16 例患者中的 15 例(93.7%,p=0.0001)BO 得到解决,OCTT 从 180 分钟显著减少至 139 分钟(SD 58.5,差异-41 分钟,p=0.0001)。35 例患者中有 21 例(60%)的血清 IL-6 水平从 41.1 降至 19pg/ml(p=0.01),10 例(28.5%)的 TNF-a 水平从 10.7 降至 5.6pg/ml(p=0.007),20 例(57%)的 LPS 水平从 7.1 降至 5.2mg/L(p=0.1)。基线或普萘洛尔治疗期间,所有患者的血清中均未检测到细菌 DNA。IP 显著降低(0.2 至 0.16,p=0.04),而 ICNC(p=0.9)、ICCM(p=0.4)和 GP(p=0.7)无明显变化。肠通透性(PI)指数(乳果糖与甘露醇比值)显著降低(0.027 至 0.02,p=0.03)。
在肝硬化伴门静脉高压患者中,普萘洛尔的使用与 BO 减少、肠道动力增加和肠道通透性改善有关。此外,大多数患者的 IL-6 和 LPS 水平在普萘洛尔治疗后降低。