Bhutani Manisha, Robinson Myra, Foureau David, Atrash Shebli, Paul Barry, Guo Fei, Grayson Jason M, Ivanina-Foureau Anna, Pineda-Roman Mauricio, Varga Cindy, Friend Reed, Ferreri Christopher J, Begic Xhevahire, Norek Sarah, Drennan Tiffany, Anderson Michelle B, Symanowski James T, Voorhees Peter M, Usmani Saad Z
Department of Hematologic Oncology and Blood Disorders, Atrium Health Levine Cancer Institute, Wake Forest University School of Medicine, Charlotte, NC.
Department of Biostatistics and Data Sciences, Atrium Health Levine Cancer Institute, Charlotte, NC.
Blood Adv. 2025 Feb 11;9(3):507-519. doi: 10.1182/bloodadvances.2024014417.
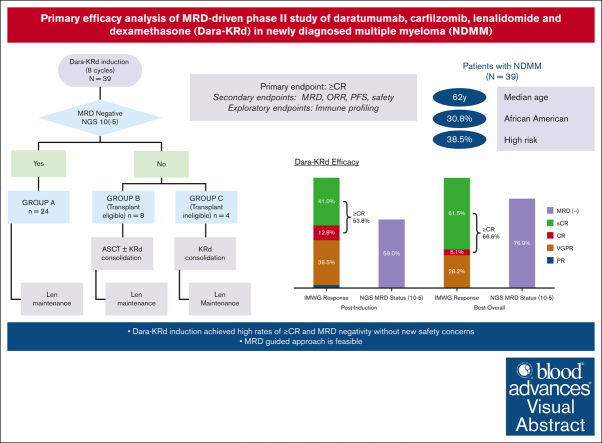
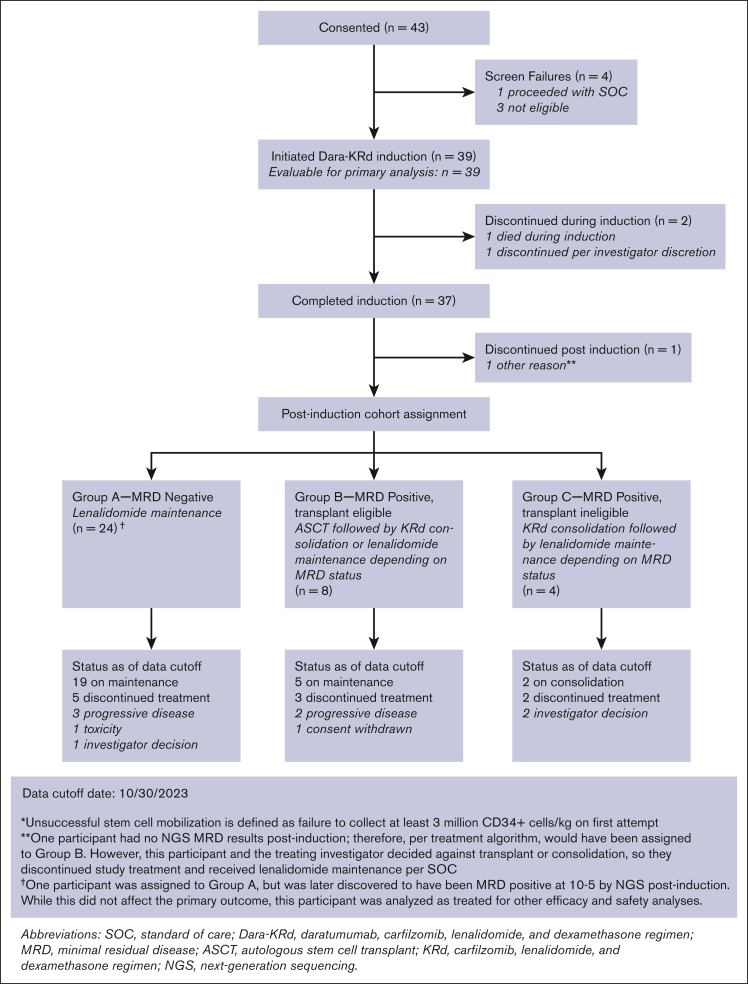
In newly diagnosed multiple myeloma (NDMM), measurable residual disease (MRD) status is prognostically important, but its role in treatment decisions remains unclear. In a phase 2 trial, we assessed daratumumab, carfilzomib, lenalidomide, and dexamethasone (Dara-KRd) induction followed by a next-generation sequencing-based MRD-adapted strategy. The primary outcome was complete response (CR) and stringent CR (≥CR) after induction. Flow cytometry was used to profile T cells. Among 39 patients, 21 (54%) achieved ≥CR after induction (P = .375), with MRD-negative rates of 59% (10-5) and 41% (10-6). Patients who were MRD-negative (n = 24, group A) received lenalidomide maintenance, showing sustained MRD negativity in 14 of 18 (77.8%) for ≥12 cycles. MRD-positive transplant-eligible patients (n = 8, group B) underwent autologous stem cell transplantation, with 62.5% converting to MRD-negative at 10-5 (37.5% at 10-6) posttransplant. MRD-positive, transplant-ineligible patients (n = 4, group C) received KRd consolidation. Best MRD-negative rates improved to 77% (10-5) and 72% (10-6). No new safety concerns were identified for Dara-KRd. With a median follow-up of 30.1 months, 3, 2, and 1 patient(s) in groups A, B, and C, respectively, have progressed or died. We observed that Dara-KRd strongly activated memory T cells, which was associated with an MRD-negative state post induction. Although the primary outcome was not met, Dara-KRd induction in NDMM achieved high ≥CR and MRD-negative rates without new safety concerns. The post induction MRD-adapted strategy deepened responses in MRD-positive patients and maintained durable MRD control in MRD-negative patients. This trial was registered at www.clinicaltrials.gov as #NCT04113018.
在新诊断的多发性骨髓瘤(NDMM)中,可测量残留病(MRD)状态具有重要的预后意义,但其在治疗决策中的作用仍不明确。在一项2期试验中,我们评估了达雷妥尤单抗、卡非佐米、来那度胺和地塞米松(Dara-KRd)诱导方案,随后采用基于下一代测序的MRD适应性策略。主要结局是诱导后完全缓解(CR)和严格完全缓解(≥CR)。采用流式细胞术分析T细胞。39例患者中,21例(54%)诱导后达到≥CR(P = 0.375),MRD阴性率分别为59%(10-5)和41%(10-6)。MRD阴性患者(n = 24,A组)接受来那度胺维持治疗,18例中有14例(77.8%)在≥12个周期内持续保持MRD阴性。符合移植条件的MRD阳性患者(n = 8,B组)接受自体干细胞移植,移植后10-5时62.5%转化为MRD阴性(10-6时为37.5%)。不符合移植条件的MRD阳性患者(n = 4,C组)接受KRd巩固治疗。最佳MRD阴性率提高到77%(10-5)和72%(10-6)。未发现Dara-KRd有新的安全问题。中位随访30.1个月,A、B、C组分别有3例、2例和1例患者进展或死亡。我们观察到Dara-KRd强烈激活记忆T细胞,这与诱导后MRD阴性状态相关。虽然未达到主要结局,但NDMM患者采用Dara-KRd诱导方案可实现较高的≥CR率和MRD阴性率,且无新的安全问题。诱导后MRD适应性策略加深了MRD阳性患者的缓解程度,并在MRD阴性患者中维持了持久的MRD控制。本试验已在www.clinicaltrials.gov注册,注册号为#NCT04113018。