Scala Raffaele, Renda Teresa, Bambina Sonia, Guidelli Luca, Arniani Stefania, Carrassa Laura, Oczkowski Simon
Pulmonology and PIMCU, Cardio-Toraco-Neurovascular Department, S. Donato Hospital, Arezzo Usl Toscana Sudest, Via Nenni, 20, Arezzo, 52100, Italy.
Demographic and Epidemiologic Section, Prevention Department, S. Donato Hospital, Arezzo Usl Toscana Sudest, Arezzo, Italy.
Pneumonia (Nathan). 2024 Nov 25;16(1):22. doi: 10.1186/s41479-024-00145-9.
Early prediction of non-invasive respiratory therapy (NIRT) failure is crucial to avoid needless prolongation of respiratory support and delayed endotracheal intubation. Data comparing the predictive value of oxygenation indices (OI) in COVID-19 receiving NIRT are scant. The aim of this monocentric retrospective study of prospectively collected data was to assess the effectiveness of different OI in predicting NIRT outcome at baseline (t0), 12 h (t12) and 24 h (t24) of treatment in hypoxemic patients with COVID-19-related pneumonia, managed in a Pulmonary Intermediate Care Unit (October 2020-June 2021).
We assessed the predictive value of SpO2/FiO2, PaO2/FiO2, standardised PaO2/FiO2 ratio (s-PaO2/FiO2), respiratory index (RI), arterial-alveolar oxygen gradient (a-ADO2), age adjusted arterial-alveolar oxygen ratio (adj-a-ADO2D). Receiver operating characteristics (ROC), AUC and best sensitivity-specificity cut-off values were calculated at t0, t12, t24. NIRT failure risk was adjusted for non-oxygenation predictors.
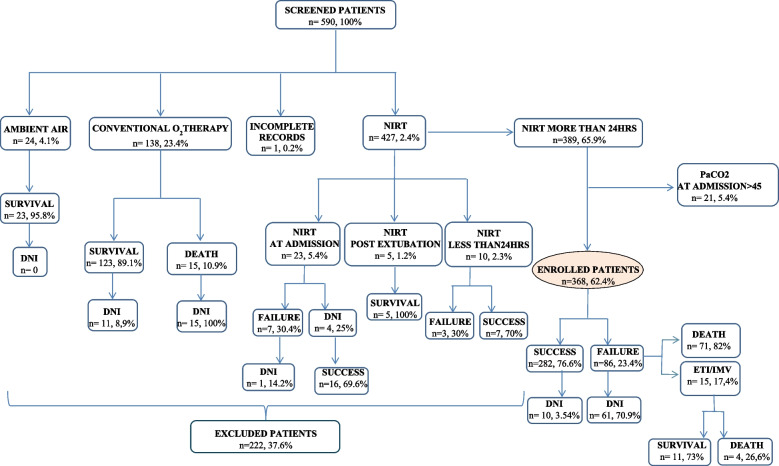
Among 590 patients with COVID-19 infection, 368 met the eligibility criteria for inclusion in the study [mean (CI95%): PaO2/FiO2 214(206,8-221,9); PaCO2 mean 32,9 mmHg,(32,4-33,4)]. NIRT failure and hospital mortality rate were 23,4% and 19,6%, respectively. Older age, male gender, agitation/confusion, need for sedation, inability to tolerate prone positioning were independent predictors of NIRT failure. SpO2/FiO2, a-ADO2 and adj-aADO2 at t12 and t24, PaO2/FiO2 and RI at t24 were associated with NIRT failure. Prognostic predictivity of OI increased from t0 to t24. Greater ROC-AUC values were obtained with SpO2/FiO2 0,662 (0,60-0,72) (t0), PaO2/FiO2 0,697 (0,63-0,76) (t12) and s-PaO2/FiO2 0,769 (0,71-0,83) (t24). NIRT failure was independently predicted by PaO2/FiO2, s-PaO2/FiO2 and RI at any observation time and by SpO2/FiO2 and O2 gradients respectively at t0 and t24. SaO2/FiO2 ≤ 300 (t0), PaO2/FiO2 ≤ 151,7 (t12) and s-PaO2/FiO2 ≤ 160,4 (t24) turned out to be the best predictors of NIRT outcome.
OI showed different effectiveness in predicting NIRT failure within 24 h of treatment in COVID-19 related pneumonia. This may be due to the multi-factorial pathophysiology of hypoxemia. Our study empathises furthermore the role of non-oxygenation-related parameters in contributing to the outcome. These findings may be useful to build a predictive model also in no COVID-19 related hypoxemic pneumonia.
无创呼吸治疗(NIRT)失败的早期预测对于避免呼吸支持的不必要延长和延迟气管插管至关重要。比较接受NIRT的2019冠状病毒病(COVID-19)患者中氧合指数(OI)预测价值的数据很少。这项对前瞻性收集的数据进行的单中心回顾性研究的目的是评估不同OI在预测2020年10月至2021年6月在肺中级护理病房接受治疗的COVID-19相关性肺炎低氧血症患者治疗基线(t0)、12小时(t12)和24小时(t24)时NIRT结果的有效性。
我们评估了血氧饱和度/吸入氧分数值(SpO2/FiO2)、动脉血氧分压/吸入氧分数值(PaO2/FiO2)、标准化动脉血氧分压/吸入氧分数值(s-PaO2/FiO2)、呼吸指数(RI)、动脉-肺泡氧梯度(a-ADO2)、年龄校正动脉-肺泡氧比值(adj-a-ADO2D)的预测价值。在t0、t12、t24计算受试者工作特征(ROC)、曲线下面积(AUC)和最佳敏感性-特异性临界值。对非氧合预测因素调整NIRT失败风险。
在590例COVID-19感染患者中,368例符合纳入研究的资格标准[均值(CI95%):PaO2/FiO2 214(206.8-221.9);动脉血二氧化碳分压均值32.9 mmHg(32.4-33.4)]。NIRT失败率和医院死亡率分别为23.4%和19.6%。年龄较大、男性、烦躁/意识模糊、需要镇静、无法耐受俯卧位是NIRT失败的独立预测因素。t12和t24时的SpO2/FiO2、a-ADO2和adj-aADO2,t24时的PaO2/FiO2和RI与NIRT失败相关。OI的预后预测性从t0到t24增加。SpO2/FiO2为0.662(0.60-0.72)(t0)、PaO2/FiO2为0.697(0.63-0.76)(t12)和s-PaO2/FiO2为0.769(0.71-0.83)(t24)时获得更大的ROC-AUC值。在任何观察时间,PaO2/FiO2、s-PaO2/FiO2和RI以及分别在t0和t24时的SpO2/FiO2和氧梯度独立预测NIRT失败。血氧饱和度/吸入氧分数值≤300(t0)、动脉血氧分压/吸入氧分数值≤151.7(t12)和标准化动脉血氧分压/吸入氧分数值≤160.4(t24)被证明是NIRT结果的最佳预测因素。
OI在预测COVID-19相关性肺炎治疗24小时内NIRT失败方面显示出不同的有效性。这可能归因于低氧血症的多因素病理生理学。我们的研究进一步强调了非氧合相关参数对结果的影响。这些发现可能有助于建立一个也适用于非COVID-19相关性低氧血症肺炎的预测模型。