Department of Pulmonology, University Hospital of Cattinara, Trieste, Italy
Department of Medical, Surgical and Health Sciences, University of Trieste, Trieste, Italy.
Eur Respir J. 2023 Apr 20;61(4). doi: 10.1183/13993003.01514-2022. Print 2023 Apr.
Dysregulated systemic inflammation is the primary driver of mortality in severe coronavirus disease 2019 (COVID-19) pneumonia. Current guidelines favour a 7-10-day course of any glucocorticoid equivalent to dexamethasone 6 mg daily. A comparative randomised controlled trial (RCT) with a higher dose and a longer duration of intervention was lacking.
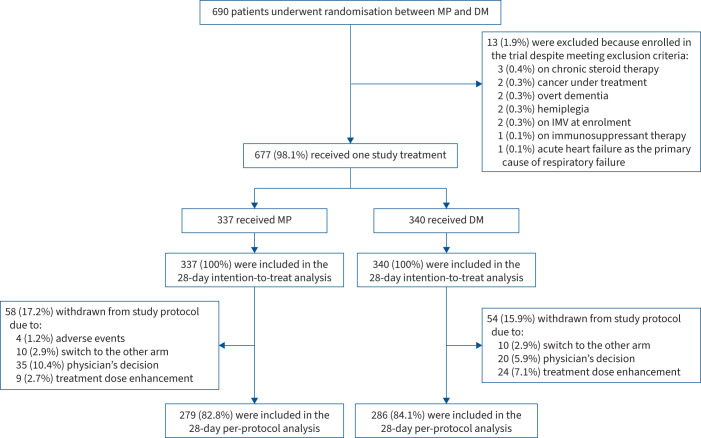
We conducted a multicentre, open-label RCT to investigate methylprednisolone 80 mg as a continuous daily infusion for 8 days followed by slow tapering dexamethasone 6 mg once daily for up to 10 days in adult patients with COVID-19 pneumonia requiring oxygen or noninvasive respiratory support. The primary outcome was reduction in 28-day mortality. Secondary outcomes were mechanical ventilation-free days at 28 days, need for intensive care unit (ICU) referral, length of hospitalisation, need for tracheostomy, and changes in C-reactive protein (CRP) levels, arterial oxygen tension/inspiratory oxygen fraction ( / ) ratio and World Health Organization Clinical Progression Scale at days 3, 7 and 14.
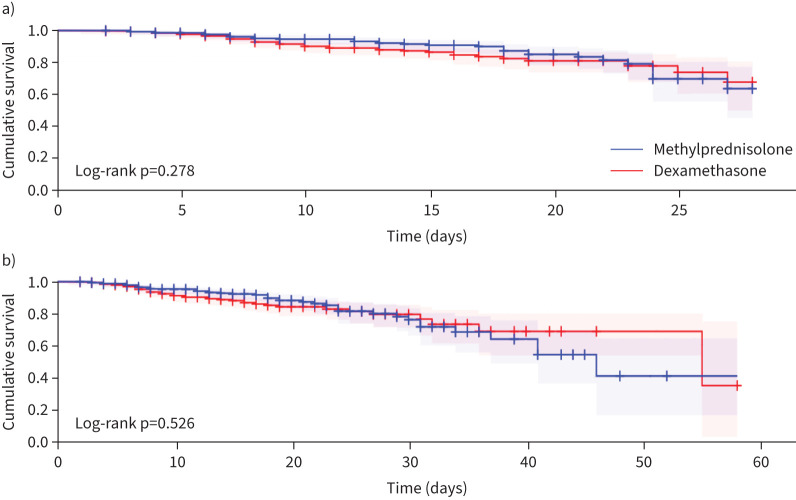
677 randomised patients were included. Findings are reported as methylprednisolone (n=337) dexamethasone (n=340). By day 28, there were no significant differences in mortality (35 (10.4%) 41 (12.1%); p=0.49) nor in median mechanical ventilation-free days (median (interquartile range (IQR)) 23 (14) 24 (16) days; p=0.49). ICU referral was necessary in 41 (12.2%) 45 (13.2%) (p=0.68) and tracheostomy in 8 (2.4%) 9 (2.6%) (p=0.82). Survivors in the methylprednisolone group required a longer median (IQR) hospitalisation (15 (11) 14 (11) days; p=0.005) and experienced an improvement in CRP levels, but not in / ratio, at days 7 and 14. There were no differences in disease progression at the prespecified time-points.
Prolonged, higher dose methylprednisolone did not reduce mortality at 28 days compared with conventional dexamethasone in COVID-19 pneumonia.
系统性炎症失调是导致严重 2019 冠状病毒病(COVID-19)肺炎患者死亡的主要原因。目前的指南主张使用任何糖皮质激素等效物,如地塞米松,7-10 天疗程。缺乏剂量更高、干预时间更长的对照随机临床试验(RCT)。
我们进行了一项多中心、开放性 RCT,以评估甲基强的松龙 80mg 持续每日输注 8 天,然后逐渐减量至地塞米松 6mg 每日一次,最长 10 天,用于需要吸氧或无创呼吸支持的 COVID-19 肺炎成年患者。主要结局为 28 天死亡率降低。次要结局为 28 天无机械通气天数、需要转入 ICU、住院时间、需要气管切开术以及第 3、7 和 14 天 C 反应蛋白(CRP)水平、动脉血氧分压/吸氧分数( / )比值和世界卫生组织临床进展量表的变化。
共纳入 677 例随机患者。结果报告为甲基强的松龙(n=337)和地塞米松(n=340)。到第 28 天,死亡率无显著差异(35(10.4%) 41(12.1%);p=0.49),机械通气无天数也无显著差异(中位数(四分位距(IQR))23(14) 24(16)天;p=0.49)。需要转入 ICU 的分别为 41(12.2%)和 45(13.2%)(p=0.68),需要气管切开术的分别为 8(2.4%)和 9(2.6%)(p=0.82)。甲基强的松龙组的幸存者需要更长的中位(IQR)住院时间(15(11) 14(11)天;p=0.005),CRP 水平在第 7 天和第 14 天有所改善,但 / 比值无差异。在预设的时间点,疾病进展无差异。
与常规地塞米松相比,COVID-19 肺炎中,延长、高剂量甲基强的松龙治疗不能降低 28 天死亡率。