From Baylor College of Medicine (S.P.L.) and the University of Texas M.D. Anderson Cancer Center (A.M.K.), Houston, the University of Texas Health San Antonio (R.S.S.) and CHRISTUS Santa Rosa Medical Center Hospital (I.M.T.), San Antonio, and the University of Texas Southwestern Medical Center, Dallas (A.I.S.) - all in Texas; Stanford University, Stanford (E.S.), Norris Comprehensive Cancer Center, University of Southern California, Los Angeles (S.D., A.S.), and City of Hope Medical Center, Duarte (S.K.P.) - all in California; SWOG Statistics and Data Management Center and Fred Hutchinson Cancer Center - both in Seattle (C.T., M.P.); the Ohio State University, Columbus (K.S.P.); the University of Chicago, Chicago (N.D.S.); McGill University Health Center, Montreal (W.K.); the Bladder Cancer Advocacy Network, SWOG Advocates, Pittsford, NY (R.B.); Oregon Health and Science University, Portland (T.M.K.); the University of Michigan, Ann Arbor (A.A.); the University of Colorado, Aurora (F.G.L.R.); Brigham and Women's Hospital, Boston (A.S.K.); Fox Chase Cancer Center, Philadelphia (D.J.C.); and Oschsner Medical Center, Jefferson, LA (D.J.C.).
N Engl J Med. 2024 Oct 3;391(13):1206-1216. doi: 10.1056/NEJMoa2401497.
Whether extended lymphadenectomy is associated with improved disease-free and overall survival, as compared with standard lymphadenectomy, among patients with localized muscle-invasive bladder cancer undergoing radical cystectomy is unclear.
We randomly assigned, in a 1:1 ratio, patients with localized muscle-invasive bladder cancer of clinical stage T2 (confined to muscle) to T4a (invading adjacent organs) with two or fewer positive nodes (N0, N1, or N2) to undergo bilateral standard lymphadenectomy (dissection of lymph nodes on both sides of the pelvis) or extended lymphadenectomy involving removal of common iliac, presciatic, and presacral nodes. Randomization was performed during surgery and stratified according to the receipt and type of neoadjuvant chemotherapy, tumor stage (T2 vs. T3 or T4a), and a Zubrod's performance-status score (0 or 1 vs. 2; assessed on a 5-point scale, with higher scores indicating greater disability). The primary outcome was disease-free survival. Overall survival and safety were also assessed.
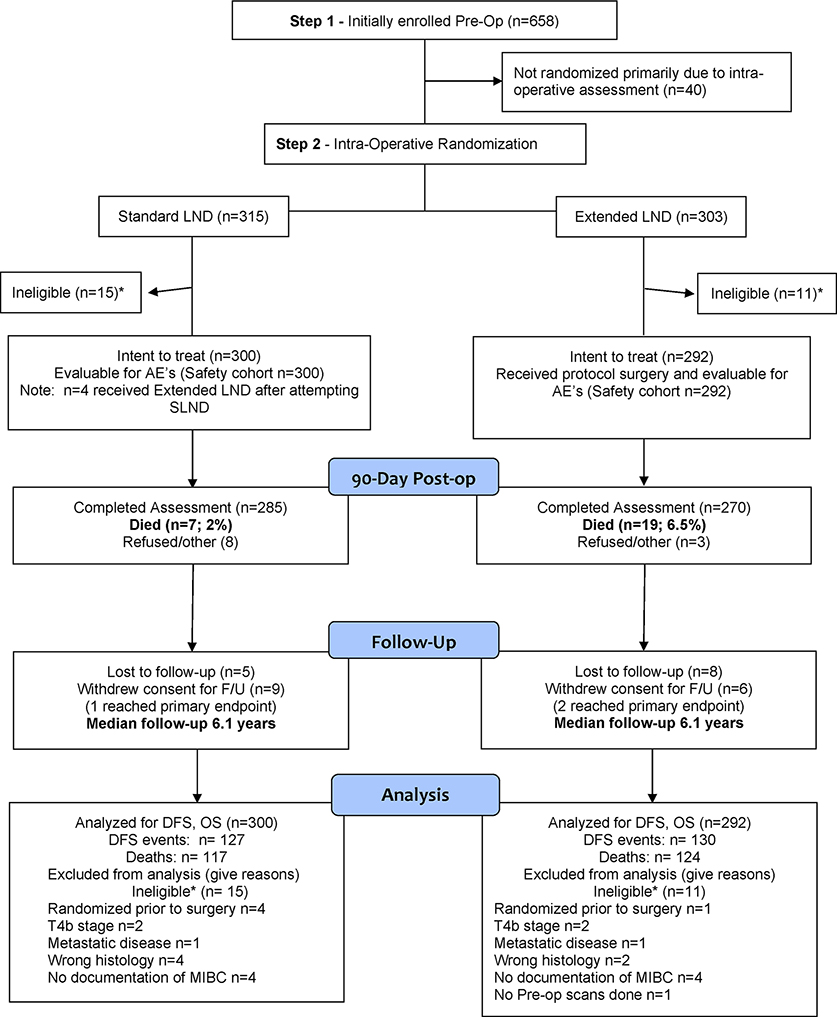
Of 658 patients who were enrolled, 592 eligible patients were randomly assigned to undergo extended lymphadenectomy (292 patients) or standard lymphadenectomy (300). Surgery was performed by 36 surgeons at 27 sites in the United States and Canada. Neoadjuvant chemotherapy had been received by 57% of the patients. At a median follow-up of 6.1 years, recurrence or death had occurred in 130 patients (45%) in the extended-lymphadenectomy group and in 127 (42%) in the standard-lymphadenectomy group, and the estimated 5-year disease-free survival was 56% and 60%, respectively (hazard ratio for recurrence or death, 1.10; 95% confidence interval [CI], 0.86 to 1.40; P = 0.45). Overall survival at 5 years was 59% in the extended-lymphadenectomy group and 63% in the standard-lymphadenectomy group (hazard ratio for death, 1.13; 95% CI, 0.88 to 1.45). Adverse events of grade 3 to 5 occurred in 157 patients (54%) in the extended-lymphadenectomy group and in 132 (44%) in the standard-lymphadenectomy group; death within 90 days after surgery occurred in 19 patients (7%) and 7 patients (2%), respectively.
As compared with standard lymphadenectomy, extended lymphadenectomy did not result in improved disease-free or overall survival among patients with muscle-invasive bladder cancer undergoing radical cystectomy and was associated with higher perioperative morbidity and mortality. (Funded by the National Cancer Institute and the Canadian Cancer Society; SWOG S1011 ClinicalTrials.gov number, NCT01224665.).
对于接受根治性膀胱切除术的局部肌层浸润性膀胱癌患者,与标准淋巴结清扫术相比,扩大淋巴结清扫术是否与改善无病生存率和总生存率相关尚不清楚。
我们以 1:1 的比例将临床分期为 T2(局限于肌肉)至 T4a(侵犯邻近器官)、有 2 个或 2 个以下阳性淋巴结(N0、N1 或 N2)的局部肌层浸润性膀胱癌患者随机分为两组,分别行双侧标准淋巴结清扫术(清扫骨盆两侧的淋巴结)或扩大淋巴结清扫术(切除髂总、坐骨和骶前淋巴结)。在手术期间进行随机分组,并根据新辅助化疗的接受情况和类型、肿瘤分期(T2 与 T3 或 T4a)以及 Zubrod 体能状态评分(0 或 1 与 2;5 分制,分数越高表示残疾程度越高)进行分层。主要终点为无病生存率。还评估了总生存率和安全性。
在纳入的 658 例患者中,592 例符合条件的患者被随机分为扩大淋巴结清扫组(292 例)或标准淋巴结清扫组(300 例)。手术由美国和加拿大 27 个地点的 36 位外科医生进行。57%的患者接受了新辅助化疗。中位随访 6.1 年后,在扩大淋巴结清扫组中有 130 例(45%)和标准淋巴结清扫组中有 127 例(42%)患者发生复发或死亡,5 年无病生存率分别为 56%和 60%(复发或死亡的风险比,1.10;95%置信区间[CI],0.86 至 1.40;P=0.45)。扩大淋巴结清扫组的 5 年总生存率为 59%,标准淋巴结清扫组为 63%(死亡风险比,1.13;95%CI,0.88 至 1.45)。在扩大淋巴结清扫组中有 157 例(54%)和标准淋巴结清扫组中有 132 例(44%)患者发生 3 级到 5 级不良事件;术后 90 天内死亡的患者分别有 19 例(7%)和 7 例(2%)。
与标准淋巴结清扫术相比,扩大淋巴结清扫术并未改善接受根治性膀胱切除术的肌层浸润性膀胱癌患者的无病生存率或总生存率,且与围手术期更高的发病率和死亡率相关。(由美国国家癌症研究所和加拿大癌症协会资助;SWOG S1011 临床试验.gov 编号,NCT01224665。)