Hospital Administration, Los Angeles General Medical Center, Los Angeles, California.
Urgent Care, Los Angeles General Medical Center, Los Angeles, California.
JAMA Netw Open. 2024 Nov 4;7(11):e2447352. doi: 10.1001/jamanetworkopen.2024.47352.
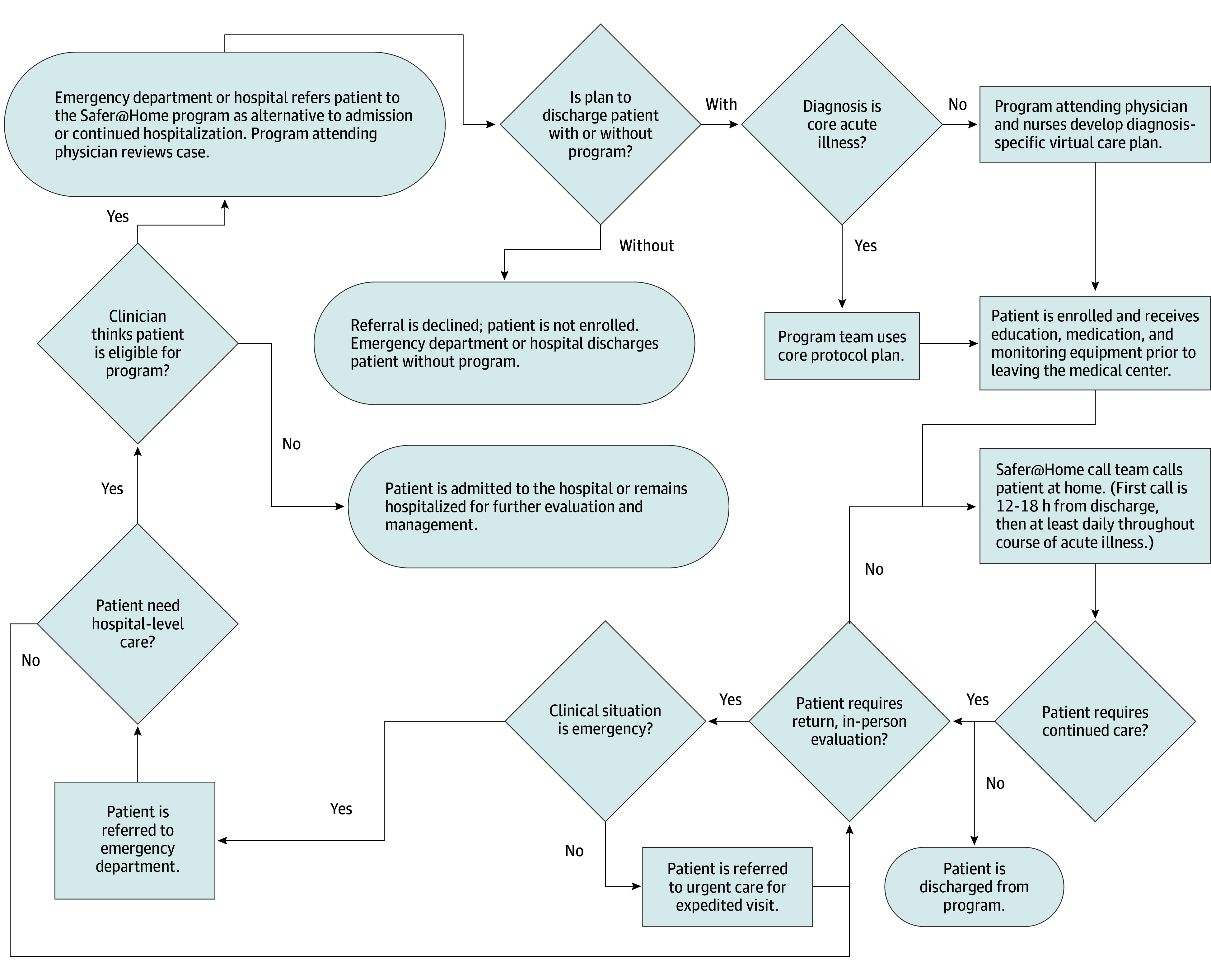
Recent evolutions in clinical care and remote monitoring suggest that some acute illnesses no longer require intravenous therapy and inpatient hospitalization.
To describe outcomes of patients receiving care in a new, outpatient, virtual, home-based acute care model called Safer@Home.
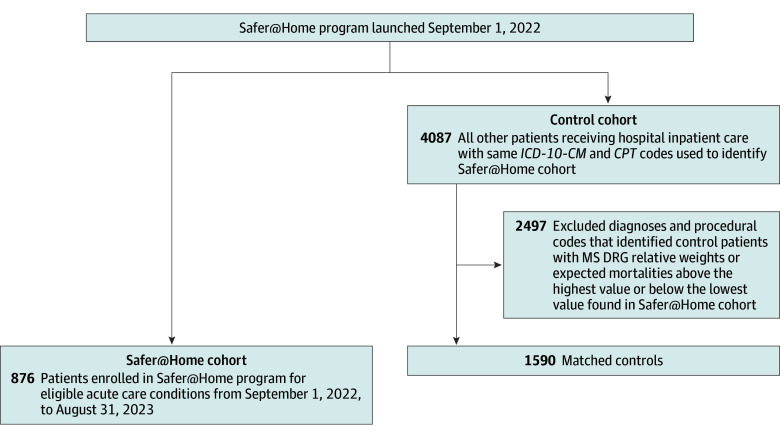
DESIGN, SETTING, AND PARTICIPANTS: This retrospective cohort analysis, conducted from September 1, 2022, through August 31, 2023, included 2466 patients treated at a safety net hospital in Los Angeles County for 10 core illnesses and 24 other acute illnesses for which patients are commonly hospitalized.
Outpatient, home-based, acute care with virtual monitoring and clinic visits in lieu of inpatient or in-home care.
The primary measure was hospital length of stay. Secondary measures included all-cause mortality, 30-day readmission, return urgent care visit rates, and return emergency department (ED) visit rates.
Safer@Home provided care to 876 patients (mean [SD] age, 54.0 [14.5] years; 541 men [61.8%]) during the study period, compared with a cohort of 1590 patients (mean [SD] age, 52.3 [19.6] years; 901 men [56.7%]) with matching diagnoses who received standard, hospital-based care. Safer@Home patients had significantly shorter mean (SD) lengths of inpatient stay than the comparison cohort (1.3 [2.0] vs 5.3 [10.4] days; P < .001), totaling 3505 bed-days avoided (mean [SD], 4.0 [10.6] bed-days saved per patient), with no significant difference in all-cause mortality at last follow-up (2.6% [23 of 876] vs 4.0% [64 of 1590]; P = .07). Safer@Home patients and control patients also had no significant difference in the proportion experiencing 30-day hospital readmission (19.9% [174 of 876] vs 16.7% [266 of 1590]; P = .06). As intended, more Safer@Home than control patients had at least one 30-day return urgent care visit (37.3% [327 of 876] vs 5.2% [82 of 1590]; P < .001). In contrast, the Safer@Home and control cohorts did not significantly differ in experiencing at least one 30-day return ED visit (15.2% [133 of 876] vs 12.5% [199 of 1590]; P = .06). Safer@Home patients had significantly fewer mean (SD) total 30-day return ED visits per patient than control patients (0.19 [0.50] vs 0.21 [0.85]; P < .001).
In this cohort study, patients receiving acute, virtual, home care with remote monitoring and as-needed return urgent care visits had markedly shorter hospital stays than patients receiving standard inpatient hospital care, with no significant increase in mortality, ED revisits, or return hospitalizations. This new care model is promising for systems that cannot staff Medicare-compliant hospital-at-home visits.
最近在临床护理和远程监测方面的发展表明,一些急性疾病不再需要静脉治疗和住院治疗。
描述在一种名为 Safer@Home 的新的、门诊、虚拟、家庭为基础的急性护理模式中接受护理的患者的结局。
设计、地点和参与者:这项回顾性队列分析于 2022 年 9 月 1 日至 2023 年 8 月 31 日进行,纳入了 2466 名在洛杉矶县的一家安全网医院接受治疗的患者,这些患者患有 10 种核心疾病和 24 种其他常见住院治疗的急性疾病。
门诊、家庭为基础的急性护理,具有虚拟监测和诊所就诊,替代住院或家庭护理。
主要测量指标是住院时间。次要测量指标包括全因死亡率、30 天再入院率、返回紧急护理就诊率和返回急诊就诊率。
在研究期间,Safer@Home 为 876 名患者(平均[标准差]年龄为 54.0[14.5]岁;541 名男性[61.8%])提供了护理,而与 1590 名匹配诊断的患者(平均[标准差]年龄为 52.3[19.6]岁;901 名男性[56.7%])相比,这些患者接受了标准的住院治疗。Safer@Home 患者的平均(标准差)住院时间明显短于对照组(1.3[2.0]比 5.3[10.4]天;P < .001),共避免了 3505 个床位天(平均[标准差]每位患者节省 4.0[10.6]个床位天),最后一次随访时全因死亡率无显著差异(2.6%[23/876]比 4.0%[64/1590];P = .07)。Safer@Home 患者和对照组患者在 30 天内再次住院的比例也没有显著差异(19.9%[174/876]比 16.7%[266/1590];P = .06)。正如预期的那样,Safer@Home 组的患者比对照组的患者有更多的至少 30 天内再次紧急护理就诊(37.3%[327/876]比 5.2%[82/1590];P < .001)。相比之下,Safer@Home 和对照组在至少 30 天内再次急诊就诊的比例没有显著差异(15.2%[133/876]比 12.5%[199/1590];P = .06)。Safer@Home 患者的平均(标准差)每位患者的 30 天内再次急诊就诊次数明显少于对照组(0.19[0.50]比 0.21[0.85];P < .001)。
在这项队列研究中,接受急性、虚拟、家庭护理,具有远程监测和按需返回紧急护理就诊的患者的住院时间明显短于接受标准住院治疗的患者,而死亡率、急诊就诊率或再次住院率没有显著增加。这种新的护理模式对于无法为符合医疗保险要求的住院患者提供服务的系统来说是很有前途的。