Alhumaid Saad, Alabdulqader Muneera, Al Alawi Zainab, Al Ghamdi Mohammed A, Alabdulmuhsin Mohammed A, Al Hassar Hassan I, Alsouaib Hussain Ahmed, Alhassan Hussain Ali, Al-Helal Hassan, Almoraihel Sameer Ahmed, Alomran Mohammed Jaber, Al-Tarfi Hassan Redha, Al-Makinah Abbas Radi, Alghareeb Tariq T, Alkhwaitem Mohammad Abdullah, Alsuliman Murtadha, Bukhamseen Ali N, Alajmi Khulood Khaled, Al Majhad Ahmed Salman, Almajhad Mariam Ali, Alhmed Ayat Hussain, Alnaim Abdulrahman A
School of Pharmacy, University of Tasmania, Hobart 7000, Australia.
Pediatric Nephrology Specialty, Pediatric Department, Medical College, King Faisal University, Al-Ahsa 31982, Saudi Arabia.
Children (Basel). 2024 Oct 28;11(11):1305. doi: 10.3390/children11111305.
PPHN is a common cause of neonatal respiratory failure and is still a serious condition that is associated with high mortality.
To analyze the clinical characteristics and outcomes of SARS-CoV-2 infection in neonates with PPHN to identify neonatal cases at risk to develop severe illness.
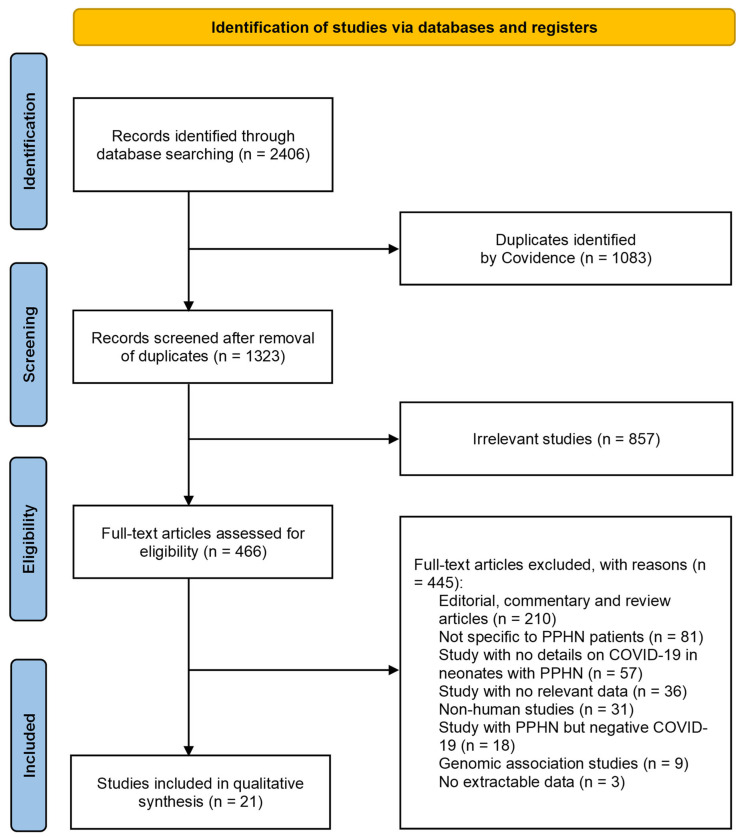
For this systematic review, we adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and searched Medline, Embase, CINAHL, and PubMed for studies on the development of COVID-19 in neonates with PPHN, published from 1 December 2019 to 29 February 2024, with an English language restriction.
Of the 2406 papers that were identified, 21 articles were included in the systematic review. Studies involving thirty-six neonates with PPHN and infected with SARS-CoV-2 were analyzed (twenty-nine survived, six died, and one is still hospitalized). The main causes of PPHN in neonates who had COVID-19 were neonatal respiratory distress syndrome (NRDS) (41.7%), meconium-stained amniotic fluid (MSAF) (16.7%), preterm premature rupture of membranes (PPROM) (11.1%), hypoxic ischemic encephalopathy (HIE) (5.5%), pneumonia (5.5%), and idiopathic (2.8%). Most of those neonates were male (33.3%), belonged to Indian ethnicity (50%), and were delivered via caesarean section (44.4%). COVID-19 in cases with PPHN commonly occurred in neonates born with a pregnancy range from 32 to <37 weeks (moderate to late preterm) (36.1%). The maternal severity of COVID-19 was reported to be severe in three cases only (8.3%); however, SARS-CoV-2 infection in neonates with PPHN was either severe (44.4%) or critical (22.2%). Most of these neonates experienced acute respiratory distress syndrome (ARDS) (58.3%). Early and late multisystem inflammatory syndrome in neonates (MIS-N) were reported in 50% and 11.1%, respectively. A high proportion of neonates were admitted to the intensive care unit (ICU) (58.3%) or needed mechanical ventilation (MV) (47.2%). Neonates with concurrent PPHN and SARS-CoV-2 infection who died had worse severity of COVID-19 [i.e., severity of COVID-19 was critical in 10% (neonates with PPHN who survived group) vs. 83.3% (neonates with PPHN who died group); = 0.026]. Neonates with PPHN and COVID-19 had a higher relative risk of death if they received more antibiotics (RR 4.14, 95% CI 0.64-6.88) and if their COVID-19 was defined as critical (RR 2.84, 95% CI 0.86-9.39). Male neonates with PPHN and COVID-19 (RR 2.60, 95% CI 0.30-1.17) and those requiring prolonged invasive positive pressure ventilation (RR 2.22, 95% CI 0.64-7.73) also showed an increased relative risk for death.
COVID-19 in neonates with PPHN is challenging and may be associated with increased mortality, severity, ICU admission, ARDS, MIS-N, and MV usage. The results should be interpreted with caution owing to the small number of studies and substantial heterogeneity and indicate a need for future research in this area. Due to its benefits, testing for SARS-CoV-2 should be encouraged for newborns with symptoms consistent with COVID-19, especially in neonates with a history of SARS-CoV-2 exposure. Effective protection measures should be implemented during delivery and post-delivery care as necessary.
持续性肺动脉高压(PPHN)是新生儿呼吸衰竭的常见原因,仍是一种与高死亡率相关的严重病症。
分析患有PPHN的新生儿感染严重急性呼吸综合征冠状病毒2(SARS-CoV-2)的临床特征和结局,以识别有发展为重症疾病风险的新生儿病例。
对于本系统评价,我们遵循系统评价和Meta分析的首选报告项目(PRISMA)指南,并检索了Medline、Embase、护理学与健康领域数据库(CINAHL)和PubMed,以查找2019年12月1日至2024年2月29日发表的关于患有PPHN的新生儿感染2019冠状病毒病(COVID-19)的研究,限定语言为英文。
在识别出的2406篇论文中,21篇文章被纳入系统评价。对36例患有PPHN且感染SARS-CoV-2的新生儿进行了分析(29例存活,6例死亡,1例仍住院)。患有COVID-19的新生儿发生PPHN的主要原因是新生儿呼吸窘迫综合征(NRDS)(41.7%)、羊水胎粪污染(MSAF)(16.7%)、胎膜早破(PPROM)(11.1%)、缺氧缺血性脑病(HIE)(5.5%)、肺炎(5.5%)和特发性(2.8%)。这些新生儿大多数为男性(33.3%),属于印度族裔(50%),且通过剖宫产分娩(44.4%)。患有PPHN的病例中,COVID-19常见于妊娠32至<37周(中度至晚期早产)出生的新生儿(36.1%)。据报道,仅3例(8.3%)产妇的COVID-19病情严重;然而,患有PPHN的新生儿感染SARS-CoV-2的病情要么严重(44.4%)要么危急(22.2%)。这些新生儿大多数经历了急性呼吸窘迫综合征(ARDS)(58.3%)。分别有50%和11.1%的新生儿报告发生了早期和晚期新生儿多系统炎症综合征(MIS-N)。很大比例的新生儿入住了重症监护病房(ICU)(58.3%)或需要机械通气(MV)(47.2%)。并发PPHN和SARS-CoV-2感染且死亡的新生儿,其COVID-19病情更严重[即,COVID-19病情危急的比例在存活的患有PPHN的新生儿组中为10%,而在死亡的患有PPHN的新生儿组中为83.3%;P = 0.026]。患有PPHN和COVID-19的新生儿如果使用了更多抗生素(相对风险4.14,95%置信区间0.64 - 6.88)以及其COVID-19被定义为危急(相对风险2.84,95%置信区间0.86 - 9.39),则死亡的相对风险更高。患有PPHN和COVID-19的男性新生儿(相对风险2.60,95%置信区间0.30 - 1.17)以及那些需要长时间有创正压通气的新生儿(相对风险2.22,95%置信区间0.64 - 7.73)死亡的相对风险也增加。
患有PPHN的新生儿感染COVID-19具有挑战性,可能与死亡率增加、病情严重程度增加、入住ICU、ARDS、MIS-N以及使用MV有关。由于研究数量少且存在大量异质性,这些结果应谨慎解读,这表明该领域需要未来的研究。鉴于其益处,对于有符合COVID-19症状的新生儿,尤其是有SARS-CoV-故在分娩期间和产后护理中应根据需要实施有效的防护措施。 2暴露史的新生儿,应鼓励进行SARS-CoV-2检测。因