Sriram Shyamkumar, Almutairi Fahad M, Albadrani Muayad
Department of Rehabilitation and Health Services, College of Health and Public Service, University of North Texas, Denton, TX 76203, USA.
Health Holding Company, Ministry of Health, Jeddah 22234, Saudi Arabia.
J Clin Med. 2024 Nov 5;13(22):6629. doi: 10.3390/jcm13226629.
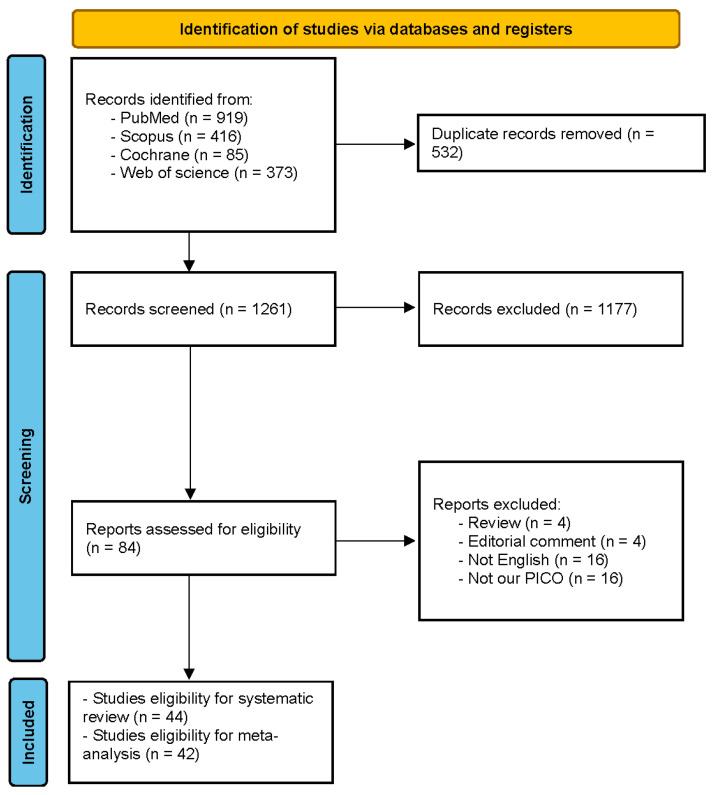
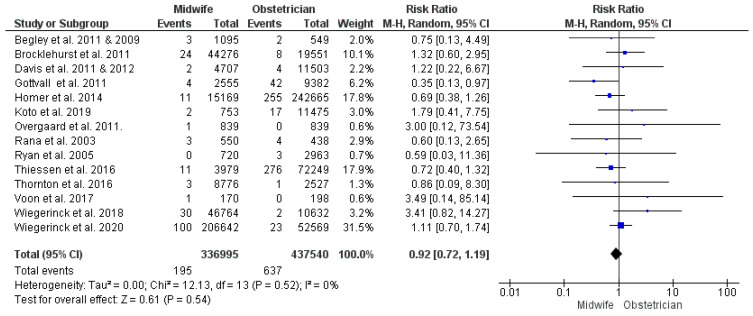
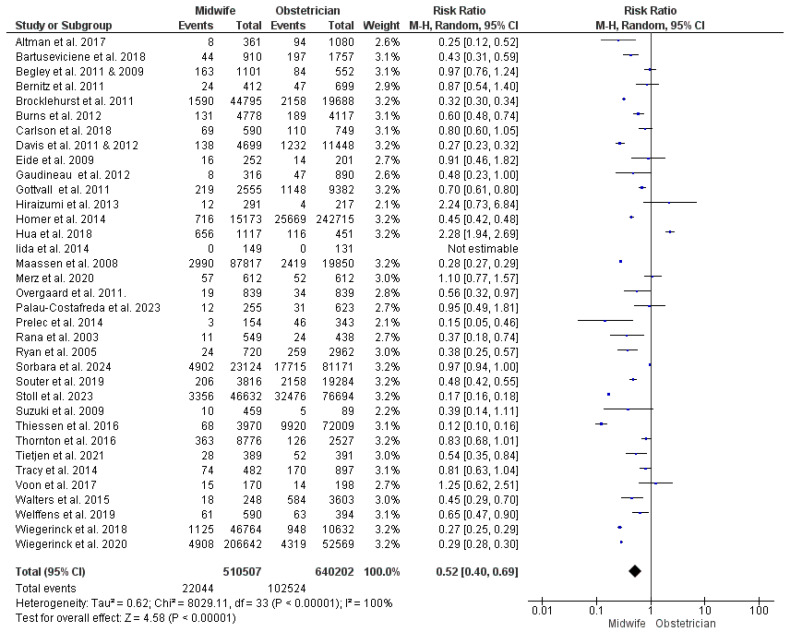
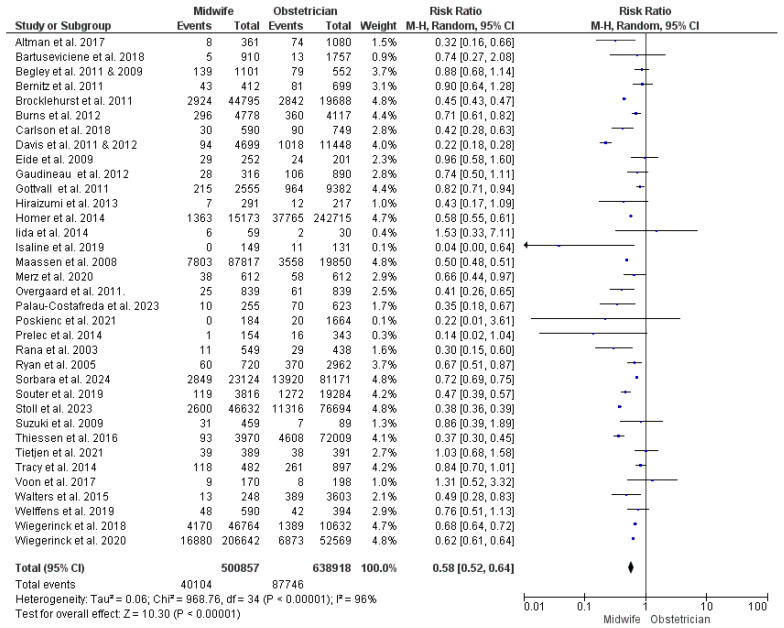
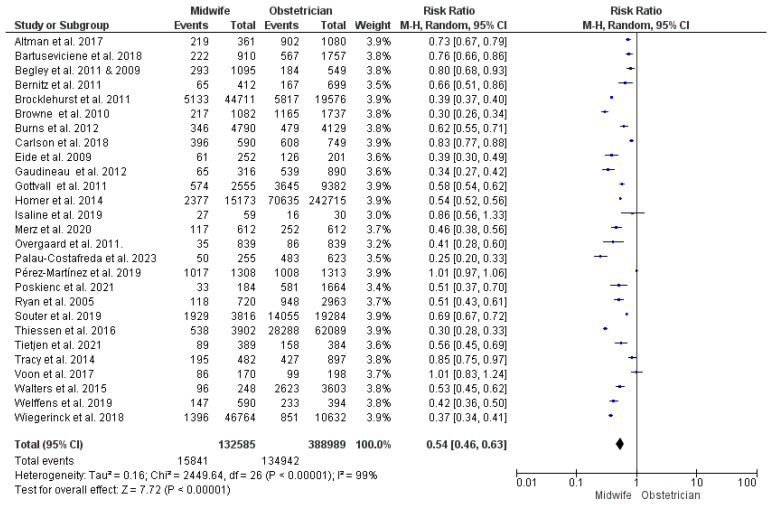
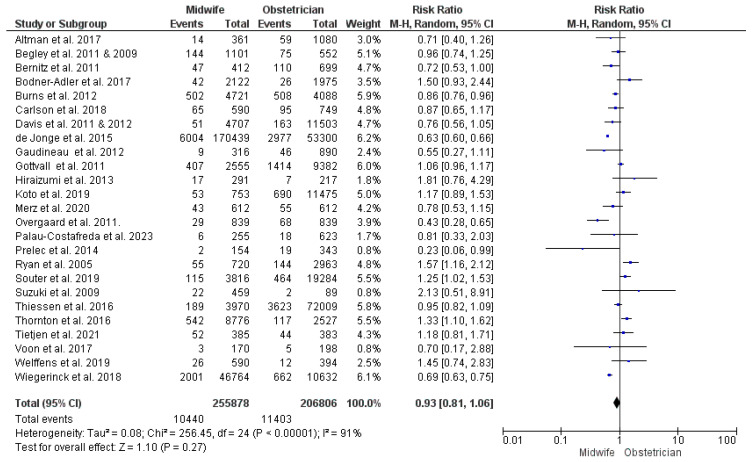
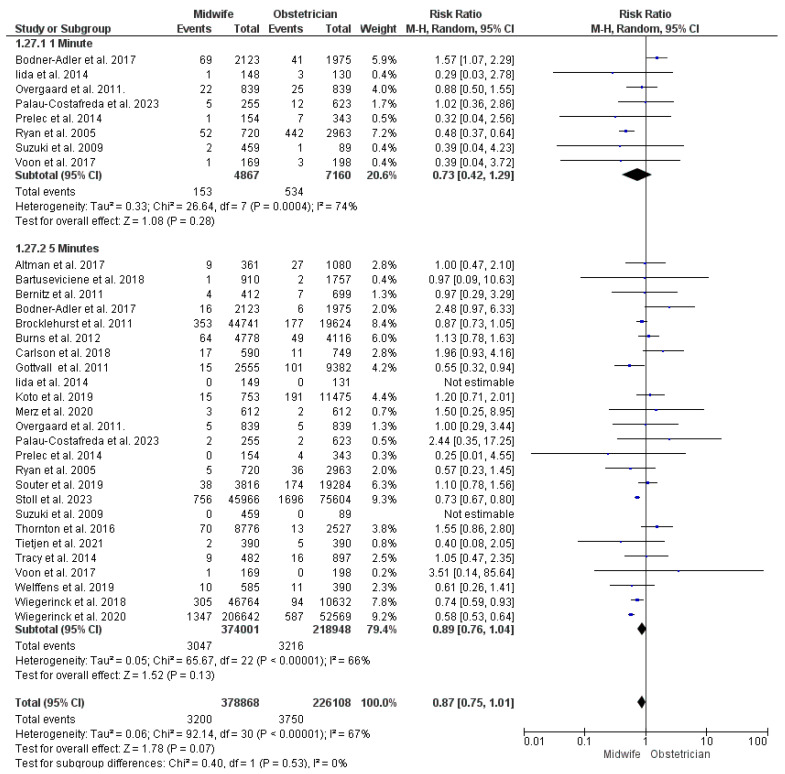
The optimum model of perinatal care for low-risk pregnancies has been a topic of debate. Obstetrician-led care tends to perform unnecessary interventions, whereas the quality of midwife-led care has been subject to debate. This review aimed to assess whether midwife-led care reduces childbirth intervention and whether this comes at the expense of maternal and neonatal wellbeing. PubMed, Scopus, Cochrane Library, and Web of Science were systematically searched for relevant studies. Studies were checked for eligibility by screening the titles, abstracts, and full texts. We performed meta-analyses using the inverse variance method using RevMan software version 5.3. We pooled data using the risk ratio and mean difference with the 95% confidence interval. This review included 44 studies with 1,397,320 women enrolled. Midwife-led care carried a lower risk of unplanned cesarean and instrumental vaginal deliveries, augmentation of labor, epidural/spinal analgesia, episiotomy, and active management of labor third stage. Women who received midwife-led care had shorter hospital stays and lower risks of infection, manual removal of the placenta, blood transfusion, and intensive care unit (ICU) admission. Furthermore, neonates delivered under midwife-led care had lower risks of acidosis, asphyxia, transfer to specialist care, and ICU admission. Postpartum hemorrhage, perineal tears, APGAR score < 7, and other outcomes were comparable between the two models of management. Midwife-led care reduced childbirth interventions with favorable maternal and neonatal outcomes in most cases. We recommend assigning low-risk pregnancies to midwife-led perinatal care in health systems with infrastructure allowing for smooth transfer when complications arise. Further research is needed to reflect the situation in low-resource countries.
低风险妊娠围产期护理的最佳模式一直是一个争论的话题。由产科医生主导的护理往往会进行不必要的干预,而由助产士主导的护理质量则一直存在争议。本综述旨在评估助产士主导的护理是否能减少分娩干预,以及这是否会以牺牲孕产妇和新生儿的健康为代价。我们系统地检索了PubMed、Scopus、Cochrane图书馆和Web of Science以查找相关研究。通过筛选标题、摘要和全文来检查研究的 eligibility。我们使用RevMan 5.3软件,采用逆方差法进行荟萃分析。我们使用风险比和平均差合并数据,并给出95%置信区间。本综述纳入了44项研究,共有1,397,320名女性参与。由助产士主导的护理发生计划外剖宫产、器械助产阴道分娩、引产、硬膜外/脊髓镇痛、会阴切开术以及第三产程积极处理的风险较低。接受助产士主导护理的女性住院时间较短,感染、人工剥离胎盘、输血和入住重症监护病房(ICU)的风险较低。此外,在助产士主导护理下分娩的新生儿发生酸中毒、窒息、转至专科护理和入住ICU的风险较低。两种管理模式下产后出血、会阴撕裂、阿氏评分<7及其他结局相当。在大多数情况下,助产士主导的护理减少了分娩干预,并取得了良好的孕产妇和新生儿结局。我们建议,在具备基础设施以便在出现并发症时能顺利转诊的卫生系统中,将低风险妊娠分配给助产士主导的围产期护理。需要进一步研究以反映资源匮乏国家的情况。