Pharmacy Department, University Hospitals Leuven, Leuven, Belgium.
Clinical Pharmacology and Pharmacotherapy, Department of Pharmaceutical and Pharmacological Sciences, KU Leuven, Leuven, Belgium.
J Med Internet Res. 2024 Nov 27;26:e55185. doi: 10.2196/55185.
Many patients do not receive a comprehensive medication reconciliation, mostly owing to limited resources. We hence need an approach to identify those patients at the emergency department (ED) who are at increased risk for clinically relevant discrepancies.
The aim of our study was to develop and externally validate a prediction model to identify patients at risk for at least 1 clinically relevant medication discrepancy upon ED presentation.
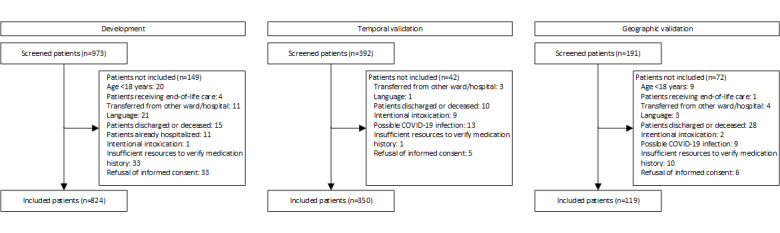
A prospective, multicenter, observational study was conducted at the University Hospitals Leuven and General Hospital Sint-Jan Brugge-Oostende AV, Belgium. Medication histories were obtained from patients admitted to the ED between November 2017 and May 2022, and clinically relevant medication discrepancies were identified. Three distinct datasets were created for model development, temporal external validation, and geographic external validation. Multivariable logistic regression with backward stepwise selection was used to select the final model. The presence of at least 1 clinically relevant discrepancy was the dependent variable. The model was evaluated by measuring calibration, discrimination, classification, and net benefit.
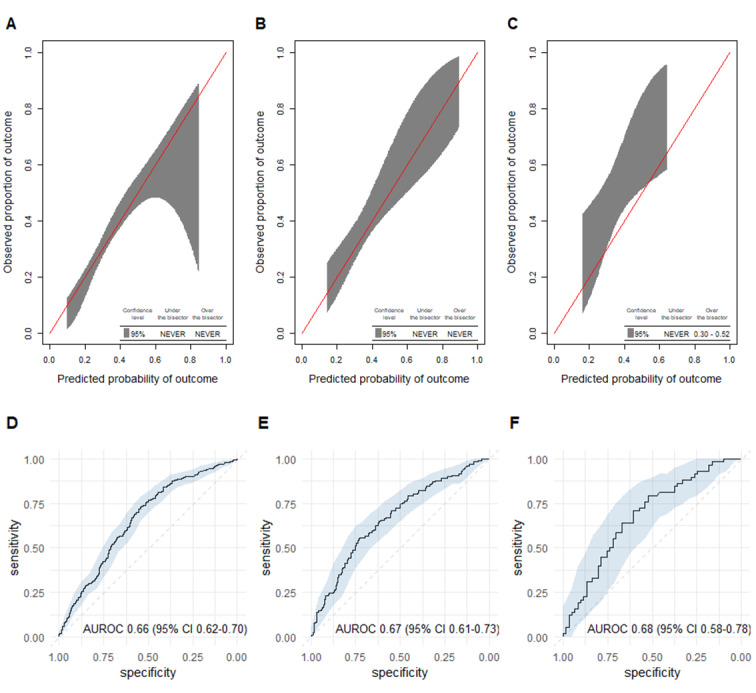
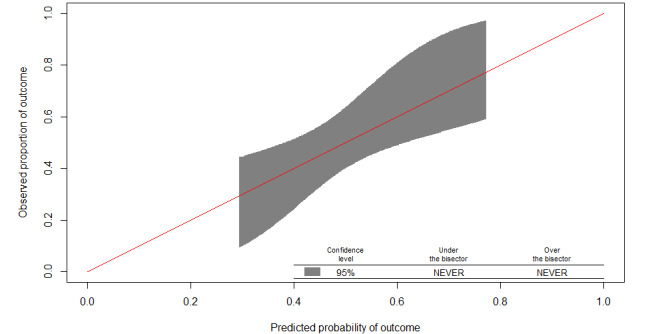
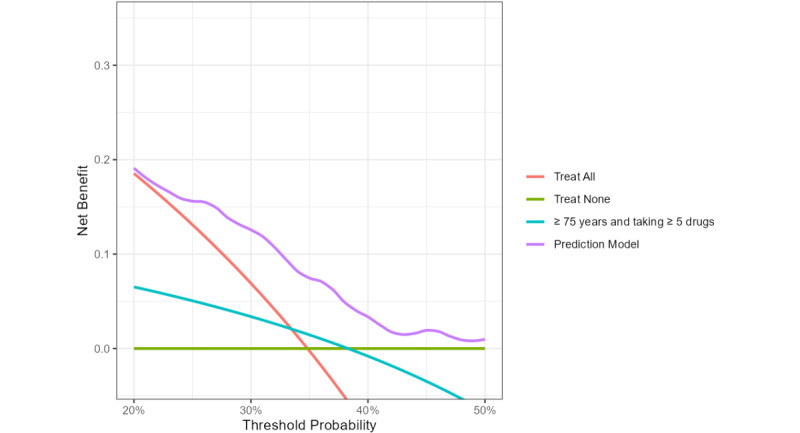
We included 824, 350, and 119 patients in the development, temporal validation, and geographic validation dataset, respectively. The final model contained 8 predictors, for example, age, residence before admission, number of drugs, and number of drugs of certain drug classes based on Anatomical Therapeutic Chemical coding. Temporal validation showed excellent calibration with a slope of 1.09 and an intercept of 0.18. Discrimination was moderate with a c-index (concordance index) of 0.67 (95% CI 0.61-0.73). In the geographic validation dataset, the calibration slope and intercept were 1.35 and 0.83, respectively, and the c-index was 0.68 (95% CI 0.58-0.78). The model showed net benefit over a range of clinically reasonable threshold probabilities and outperformed other selection criteria.
Our software-implemented prediction model shows moderate performance, outperforming random or typical selection criteria for medication reconciliation. Depending on available resources, the probability threshold can be customized to increase either the specificity or the sensitivity of the model.
许多患者并未接受全面的药物重整,这主要是由于资源有限。因此,我们需要一种方法来识别急诊科(ED)中那些存在临床相关差异风险较高的患者。
本研究旨在开发并外部验证一种预测模型,以识别 ED 就诊时至少存在 1 种临床相关药物差异的风险患者。
这是一项在比利时鲁汶大学医院和圣让-布鲁日-奥斯坦德综合医院进行的前瞻性、多中心、观察性研究。从 2017 年 11 月至 2022 年 5 月期间入住 ED 的患者中获取药物史,并确定临床相关药物差异。为模型开发、时间外部验证和地理外部验证创建了三个不同的数据集。使用向后逐步选择的多变量逻辑回归选择最终模型。至少存在 1 种临床相关差异的存在是因变量。通过测量校准、区分度、分类和净效益来评估模型。
我们分别纳入了 824 例、350 例和 119 例患者用于开发、时间验证和地理验证数据集。最终模型包含 8 个预测因素,例如年龄、入院前居住地、药物数量和基于解剖治疗化学编码的特定药物类别的药物数量。时间验证显示出极好的校准,斜率为 1.09,截距为 0.18。区分度为中度,C 指数(一致性指数)为 0.67(95%CI 0.61-0.73)。在地理验证数据集中,校准斜率和截距分别为 1.35 和 0.83,C 指数为 0.68(95%CI 0.58-0.78)。该模型在一系列合理的临床阈值概率下显示出净效益,并优于其他选择标准。
我们的软件实现预测模型表现出中等性能,优于药物重整的随机或典型选择标准。根据可用资源,可以定制概率阈值以提高模型的特异性或敏感性。