Department of Thoracic Surgery, Kanazawa Medical University, Uchinada, Ishikawa, Japan.
Am J Case Rep. 2024 Nov 30;25:e944997. doi: 10.12659/AJCR.944997.
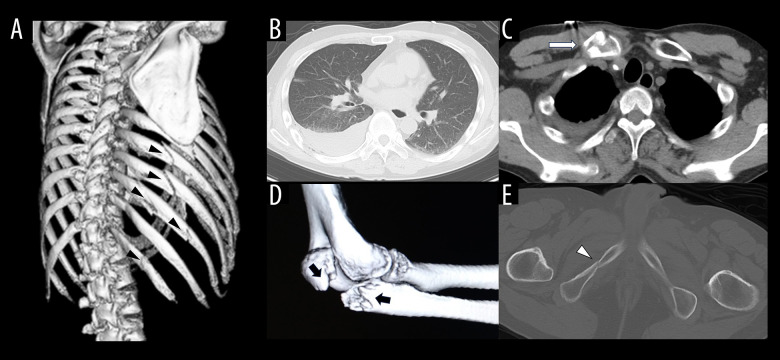
BACKGROUND Coagulopathy caused by trauma itself is defined as trauma-induced coagulopathy (TIC). The pathophysiology of TIC is considered to consist of coagulation activation, hyperfibrinolysis, and consumption coagulopathy, similar to disseminated intravascular coagulation (DIC). This report describes a 68-year-old man with a history of epilepsy presenting with TIC associated with multiple traumatic fractures and hemothorax. CASE REPORT A 68-year-old man with a history of epilepsy fell while working on a second-floor roof and had right rib fractures (6th to 12th rib), right hemothorax, right clavicle fracture, right elbow fracture, and pelvic fractures. The right hemothorax became exacerbated and he went into shock. We performed the emergency surgery 5 hours after the trauma. Although circulation dynamics became stable and the discharge of chest drainage became thinned at postoperative day (POD) 1 while administering blood transfusions and tranexamic acid, hemoglobin remained below 8 g/dl, platelet count was below 60 000/µl, and prothrombin time - international normalized ratio (1.22) remained prolonged. Furthermore, the right hemothorax became exacerbated and re-operation was performed on the evening of POD2. Oozing hemorrhages from multiple rib fractures were observed. Although hemostatic management was performed with electrocautery and ultrasound energy devices, the hemorrhage could not be completely managed, so hemostasis was secured using hemostatic materials. CONCLUSIONS The pathophysiologic mechanism of TIC has been emphasized as being different from that of DIC, and management of severe traumatic patients with TIC should be based on an understanding of the pathophysiology of TIC.
背景
由创伤本身引起的凝血功能障碍被定义为创伤诱导的凝血障碍(TIC)。TIC 的病理生理学被认为包括凝血激活、纤维蛋白溶解亢进和消耗性凝血障碍,类似于弥散性血管内凝血(DIC)。本报告描述了一位 68 岁有癫痫病史的男性患者,他因多发创伤性骨折和血胸并发 TIC。
病例报告
一位 68 岁有癫痫病史的男性患者在二楼屋顶工作时摔倒,导致右侧肋骨骨折(第 6 至 12 肋骨)、右侧血胸、右侧锁骨骨折、右侧肘部骨折和骨盆骨折。右侧血胸加重,出现休克。我们在创伤后 5 小时进行了紧急手术。虽然在输血和氨甲环酸治疗的情况下,循环动力学在术后第 1 天(POD1)变得稳定,胸腔引流的排出也变稀薄,但血红蛋白仍低于 8g/dl,血小板计数低于 60000/µl,凝血酶原时间-国际标准化比值(1.22)仍延长。此外,右侧血胸加重,在 POD2 晚上再次进行手术。观察到多发肋骨骨折处有渗血。虽然用电烙术和超声能量装置进行了止血管理,但出血仍无法完全控制,因此使用止血材料来止血。
结论
TIC 的病理生理机制已被强调不同于 DIC,对 TIC 严重创伤患者的管理应基于对 TIC 病理生理学的理解。