Llop Maria, Gómez-García Ignacio, Gratacós Jordi, Villoria Albert, Calvet Joan, Moreno Mireia, Arévalo Marta, Cabanillas-Paredes Montserrat, Collantes-Estévez Eduardo, Vazquez-Mellado Janitzia, López-Medina Clementina
Department of Rheumatology, Parc Taulí Hospital Universitari, Institut d'Investigació i Innovació Parc Taulí (I3PT-CERCA), Universitat Autònoma de Barcelona, Sabadell, Barcelona, Spain.
Department of Rheumatology, Hospital Universitario Reina Sofía/IMIBIC/Universidad de Córdoba, Córdoba, Spain.
Ther Adv Musculoskelet Dis. 2024 Nov 30;16:1759720X241303316. doi: 10.1177/1759720X241303316. eCollection 2024.
Inflammatory bowel disease (IBD) affects 5%-10% of ankylosing spondylitis (AS) patients. Prior data suggest AS patients with IBD may have more severe disease and lower HLA-B27 prevalence. Yet, little is known about potential distinctions in AS with IBD compared to those without IBD.
To investigate the clinical characteristics and radiographic differences between patients with (AS) with and without concurrent IBD.
This multicenter, observational, cross-sectional study included patients meeting European Spondyloarthropathy Study Group criteria from the Registry of Spondyloarthritis of Spanish Rheumatology (REGISPONSER) and Ibero-American Registry of Spondyloarthropathies (RESPONDIA) registries.
Characteristics and disease burden were compared between patients with and without IBD. Multivariate logistic regression identified factors independently associated with IBD presence in patients with AS.
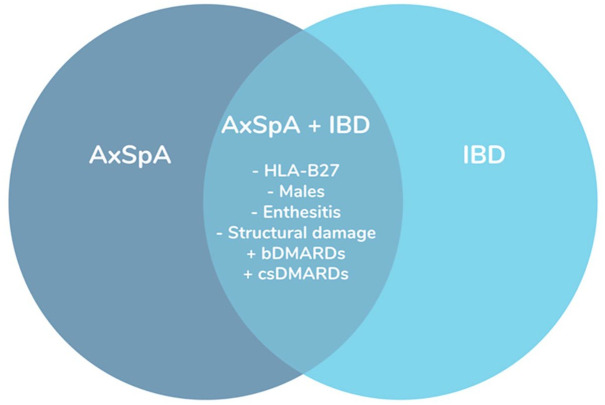
We included a total of 2766 patients with AS (1254 from REGISPONSER and 1512 from RESPONDIA), among whom 142 patients (5.13%) presented with concomitant IBD. AS patients with concurrent IBD were less frequently male, had a lower prevalence of HLA-B27 positivity, experienced a lower prolonged diagnostic delay, had a lower frequency of enthesitis, and received more commonly intensified treatment compared to those without IBD. In terms of structural damage, the Bath Ankylosing Spondylitis Radiology Index (BASRI) score for the sacroiliac joints (SIJs), cervical spine, and lumbar spine was lower in patients with AS and IBD than in those without IBD. In the multivariable analysis, the presence of IBD was significantly associated with a lower prevalence of HLA-B27 and enthesitis, with odds ratios (OR) of 0.32 (95% confidence interval (CI): 0.20-0.52) and 0.58 (95% CI: 0.33-0.97), respectively. Furthermore, structural damage in SIJs (BASRI) was significantly decreased in patients with IBD, with an OR of 0.79 (95% CI: 0.64-0.99).
The presence of IBD in AS is associated with lower HLA-B27 positivity, less enthesitis, and less radiographic damage in this large population study.
炎症性肠病(IBD)影响5%-10%的强直性脊柱炎(AS)患者。既往数据表明,合并IBD的AS患者可能病情更严重,HLA-B27阳性率更低。然而,与未合并IBD的AS患者相比,合并IBD的AS患者的潜在差异鲜为人知。
研究合并和未合并IBD的AS患者的临床特征和影像学差异。
这项多中心、观察性横断面研究纳入了来自西班牙风湿病脊柱炎登记处(REGISPONSER)和伊比利亚-美洲脊柱炎登记处(RESPONDIA)登记系统中符合欧洲脊柱关节炎研究组标准的患者。
比较合并和未合并IBD患者的特征和疾病负担。多因素逻辑回归分析确定与AS患者合并IBD独立相关的因素。
我们共纳入了2766例AS患者(1254例来自REGISPONSER,1512例来自RESPONDIA),其中142例(5.13%)合并IBD。与未合并IBD的患者相比,合并IBD的AS患者男性比例较低,HLA-B27阳性率较低,诊断延迟时间较短,附着点炎发生率较低,强化治疗的频率较高。在结构损伤方面,合并IBD的AS患者骶髂关节(SIJ)、颈椎和腰椎的巴斯强直性脊柱炎放射学指数(BASRI)评分低于未合并IBD的患者。在多变量分析中,IBD的存在与HLA-B27阳性率较低和附着点炎显著相关,比值比(OR)分别为0.32(95%置信区间(CI):0.20-0.52)和0.58(95%CI:0.33-0.97)。此外,IBD患者SIJ的结构损伤(BASRI)显著降低,OR为0.79(95%CI:0.64-0.99)。
在这项大型人群研究中,AS患者合并IBD与较低的HLA-B27阳性率、较少的附着点炎和较少的影像学损伤相关。