Kwan Jennifer M, Shen Miles, Akhlaghi Narjes, Hu Jiun-Ruey, Mora Ruben, Cross James L, Jiang Matthew, Mankbadi Michael, Wang Peter, Zaman Saif, Lee Seohyuk, Im Yunju, Feher Attila, Liu Yi-Hwa, Ma Shuangge S, Tao Weiwei, Wei Wei, Baldassarre Lauren A
Section of Cardiovascular Medicine, Yale University School of Medicine, New Haven, Connecticut, United States of America.
Yale University School of Medicine, New Haven, Connecticut, United States of America.
PLoS One. 2024 Dec 2;19(12):e0314555. doi: 10.1371/journal.pone.0314555. eCollection 2024.
There is an urgent need to better understand the diverse presentations, risk factors, and outcomes of immune checkpoint inhibitor (ICI)-associated cardiovascular toxicity. There remains a lack of consensus surrounding cardiovascular screening, risk stratification, and clinical decision-making in patients receiving ICIs.
We conducted a single center retrospective cohort study including 2165 cancer patients treated with ICIs between 2013 and 2020. The primary outcome was adverse cardiovascular events (ACE): a composite of myocardial infarction, coronary artery disease, stroke, peripheral vascular disease, arrhythmias, heart failure, valvular disease, pericardial disease, and myocarditis. Secondary outcomes included all-cause mortality and the individual components of ACE. We additionally conducted an imaging substudy examining imaging characteristics from echocardiography (echo) and cardiac magnetic resonance (CMR) imaging.
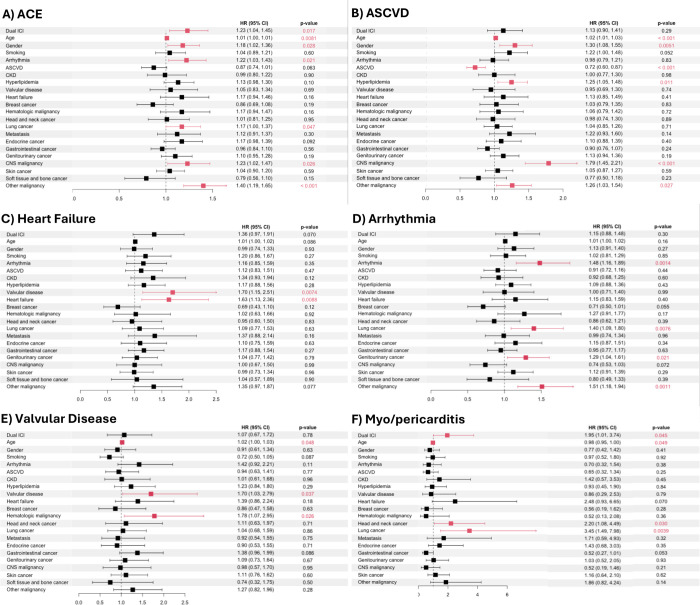
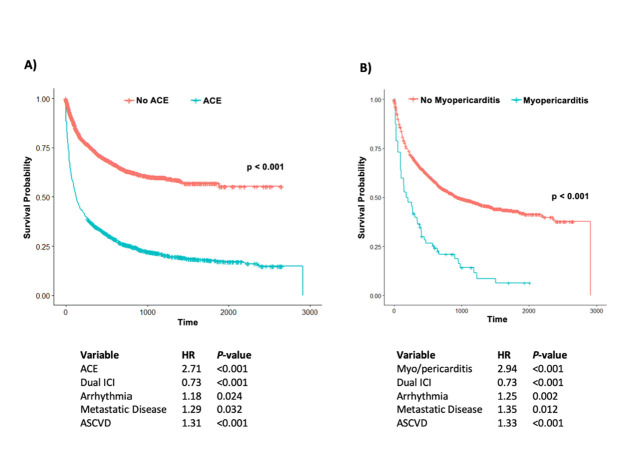
In our cohort, 44% (n = 962/2165) of patients experienced ACE. In a multivariable analysis, dual ICI therapy (hazard ratio [HR] 1.23, confidence interval [CI] 1.04-1.45), age (HR 1.01, CI 1.00-1.01), male sex (HR 1.18, CI 1.02-1.36), prior arrhythmia (HR 1.22, CI 1.03-1.43), lung cancer (HR 1.17, CI 1.01-1.37), and central nervous system (CNS) malignancy (HR 1.23, CI 1.02-1.47), were independently associated with increased ACE. ACE was independently associated with a 2.7-fold increased risk of mortality (P<0.001). Dual ICI therapy was also associated with a 2.0-fold increased risk of myo/pericarditis (P = 0.045), with myo/pericarditis being associated with a 2.9-fold increased risk of mortality (P<0.001). However, the cardiovascular risks of dual ICI therapy were offset by its mortality benefit, with dual ICI therapy being associated with a ~25% or 1.3-fold decrease in mortality. Of those with echo prior to ICI initiation, 26% (n = 115/442) had abnormal left ventricular ejection fraction or global longitudinal strain, and of those with echo after ICI initiation, 28% (n = 207/740) had abnormalities. Of those who had CMR imaging prior to ICI initiation, 43% (n = 9/21) already had left ventricular dysfunction, 50% (n = 10/20) had right ventricular dysfunction, 32% (n = 6/19) had left ventricular late gadolinium enhancement, and 9% (n = 1/11) had abnormal T2 imaging.
Dual ICI therapy, prior arrhythmia, older age, lung and CNS malignancies were independently associated with an increased risk of ACE, and dual ICI therapy was also independently associated with an increased risk of myo/pericarditis, highlighting the utmost importance of cardiovascular risk factor optimization in this particularly high-risk population. Fortunately, the occurrence of myo/pericarditis was relatively uncommon, and the overall cardiovascular risks of dual ICI therapy appeared to be offset by a significant mortality benefit. The use of multimodal cardiac imaging can be helpful in stratifying risk and guiding preventative cardiovascular management in patients receiving ICIs.
迫切需要更好地了解免疫检查点抑制剂(ICI)相关心血管毒性的多样表现、危险因素及结局。在接受ICI治疗的患者中,关于心血管筛查、风险分层及临床决策仍缺乏共识。
我们进行了一项单中心回顾性队列研究,纳入了2013年至2020年间接受ICI治疗的2165例癌症患者。主要结局为不良心血管事件(ACE):包括心肌梗死、冠状动脉疾病、中风、外周血管疾病、心律失常、心力衰竭、瓣膜病、心包疾病及心肌炎的综合指标。次要结局包括全因死亡率及ACE的各个组成部分。我们还进行了一项影像学亚研究,检查超声心动图(echo)和心脏磁共振(CMR)成像的影像学特征。
在我们的队列中,44%(n = 962/2165)的患者发生了ACE。在多变量分析中,双联ICI治疗(风险比[HR] 1.23,置信区间[CI] 1.04 - 1.45)、年龄(HR 1.01,CI 1.00 - 1.01)、男性(HR 1.18,CI 1.02 - 1.36)、既往心律失常(HR 1.22,CI 1.03 - 1.43)、肺癌(HR 1.17,CI 1.01 - 1.37)及中枢神经系统(CNS)恶性肿瘤(HR 1.23,CI 1.02 - 1.47)与ACE增加独立相关。ACE与死亡风险增加2.7倍独立相关(P<0.001)。双联ICI治疗还与心肌/心包炎风险增加2.0倍相关(P = 0.045),心肌/心包炎与死亡风险增加2.9倍相关(P<0.001)。然而,双联ICI治疗的心血管风险被其降低死亡率的益处所抵消,双联ICI治疗与死亡率降低约25%或1.3倍相关。在ICI开始前进行echo检查的患者中,26%(n = 115/442)左心室射血分数或整体纵向应变异常,在ICI开始后进行echo检查的患者中,28%(n = 207/740)有异常。在ICI开始前进行CMR成像的患者中,43%(n = 9/21)已有左心室功能障碍,50%(n = 10/20)有右心室功能障碍,32%(n = 6/19)有左心室晚期钆增强,9%(n = 1/11)有异常T2成像。
双联ICI治疗、既往心律失常、老年、肺癌及CNS恶性肿瘤与ACE风险增加独立相关,双联ICI治疗还与心肌/心包炎风险增加独立相关,突出了在这个特别高危人群中优化心血管危险因素的至关重要性。幸运的是,心肌/心包炎的发生相对不常见,双联ICI治疗的总体心血管风险似乎被显著的死亡率益处所抵消。使用多模态心脏成像有助于对接受ICI治疗的患者进行风险分层并指导预防性心血管管理。