Gismondi Alice, Frediani Simone, Pardi Valerio, Pietro Aloi Ivan, Bertocchini Arianna, Accinni Antonella, Inserra Alessandro
General and Thoracic Pediatric Surgery Unit, Bambino Gesù Children's Hospital, IRCCS, Rome, Italy.
Front Pediatr. 2024 Nov 19;12:1431590. doi: 10.3389/fped.2024.1431590. eCollection 2024.
Hemoptysis is an alarming clinical presentation caused by a vast number of primitive conditions (infectious, malignancies, malformations, vasculitis). However, at the root of hemoptysis, there is always a "noxa patogena" altering vessel structure, usually bronchial arteries, which are characterized by high pressure. Bronchial artery embolization (BAE) is the first-line treatment for hemoptysis for its technical and clinical success, although the long-term overall outcome is not equally adequate.
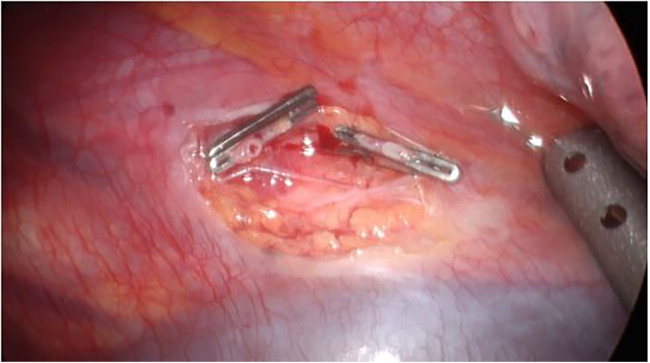
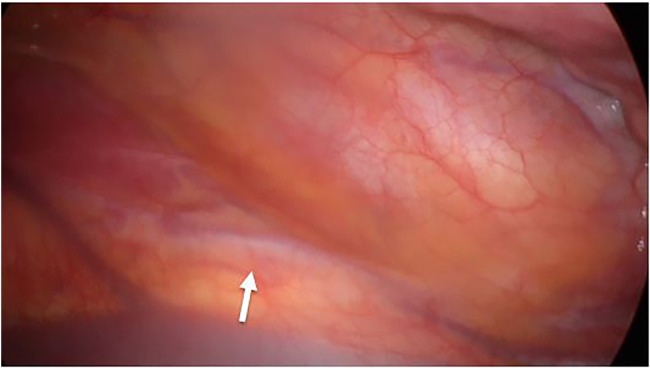
A 12-year-old boy was referred to our hospital for massive hemoptysis after a history of recurrent episodes since the age of 3. The patient had been diagnosed with bilateral and widespread bronchial artery hypertrophy at another hospital and treated with several BAE procedures. We performed BAE to stabilize the child as well as an angio-CT scan, which confirmed the presence of the recently placed coil to embolize a hypertrophic bronchial arteriosus branch originating from the left thyrocervical trunk and directed to the right lower lobe. Results of previous embolization (metal coils) were found at the origin of the right inferior thyroid artery and the right costo-cervical trunk. After 21 months since his first admission to our hospital, the patient was transferred by air ambulance for a massive hemoptysis recurrence. Further BAE of the previously coiled vessel coming from the right succlavia (and right inferior thyroid artery) was impossible to perform due to the presence of the coils positioned in the past. A thoracoscopic approach was chosen: the previously identified anomalous vessel was isolated and ligated using double metal clips, two on both the proximal and distal sides. Accurate exploration of the thoracic cavity was accomplished, verifying the absence of collateral vessels coming from the diaphragmatic side. The patient was discharged in four days in good clinical.
Although bare-minimum invasive embolism (BAE) is still the gold standard for treatment, there are situations when it may not produce the desired clinical outcome and increase the risk of rebleeding. In these situations, minimally invasive surgical procedures using a videothoracoscopic approach can be beneficial if there is a suspicion of an aberrant vessel on a DSA or CT scan.
咯血是一种由大量原发性疾病(感染、恶性肿瘤、畸形、血管炎)引起的令人担忧的临床表现。然而,咯血的根本原因始终是一种改变血管结构的“致病因素”,通常是支气管动脉,其特点是压力高。支气管动脉栓塞术(BAE)因其技术和临床成功率,是咯血的一线治疗方法,尽管长期总体疗效并不理想。
一名12岁男孩因自3岁起反复发作咯血病史,被转诊至我院。该患者在另一家医院被诊断为双侧广泛性支气管动脉肥大,并接受了多次BAE治疗。我们进行了BAE以稳定患儿病情,并进行了血管CT扫描,证实了最近放置的线圈栓塞了起源于左甲状腺颈干并指向右下叶的肥大支气管动脉分支。在右甲状腺下动脉和右肋颈干的起始处发现了先前栓塞(金属线圈)的结果。自首次入院21个月后,患者因大量咯血复发通过空中救护车转诊。由于过去放置的线圈存在,无法对来自右锁骨下(和右甲状腺下动脉)的先前盘绕血管进行进一步的BAE。选择了胸腔镜方法:分离先前确定的异常血管,使用双金属夹在近端和远端两侧各夹两个进行结扎。完成了胸腔的精确探查,确认没有来自膈肌侧的侧支血管。患者在四天后临床情况良好出院。
尽管微创栓塞术(BAE)仍然是治疗的金标准,但在某些情况下,它可能无法产生预期的临床效果,并增加再出血的风险。在这些情况下,如果在DSA或CT扫描中怀疑有异常血管,采用电视胸腔镜方法的微创手术可能是有益的。