MacManus Michael P, Seymour John F, Tsang Hennes, Fisher Richard, Keane Colm, Sabdia Muhammed B, Law Soi C, Gunawardana Jay, Nath Karthik, Kazakoff Stephen H, Marques-Piubelli Mario L, Duenas Daniela E, Green Michael R, Roos Daniel, O'Brien Peter, McCann Andrew, Tsang Richard, Davis Sidney, Christie David, Cheah Chan, Amanuel Benhur, Cochrane Tara, Butler Jason, Johnston Anna, Shanavas Mohamed, Li Li, Vajdic Claire, Kridel Robert, Shelton Victoria, Hershenfield Samantha, Baetz Tara, Lebrun David, Johnson Nathalie, Brodtkorb Marianne, Ludvigsen Maja, d'Amore Francesco, Thompson Ella R, Blombery Piers, Gandhi Maher K, Tobin Joshua W D
Peter MacCallum Cancer Institute, Melbourne, VIC, Australia; University of Melbourne, VIC, Australia.
Peter MacCallum Cancer Institute, Melbourne, VIC, Australia; University of Melbourne, VIC, Australia.
EBioMedicine. 2024 Dec;110:105468. doi: 10.1016/j.ebiom.2024.105468. Epub 2024 Dec 3.
We report extended follow-up of TROG99.03, a randomised phase III trial in early-stage follicular lymphoma (ESFL) including new information on the role of adjuvant rituximab and translational studies.
Patients with ESFL were randomised to involved field radiotherapy (IFRT) or IFRT plus 6-cycles cyclophosphamide/vincristine/prednisolone (IFRT + CVP). From 2006 rituximab was added to IFRT + CVP (IFRT + R-CVP). Clinical and multi-omic parameters were evaluated. Findings were validated in two independent ESFL cohorts (99 and 60 patients respectively).
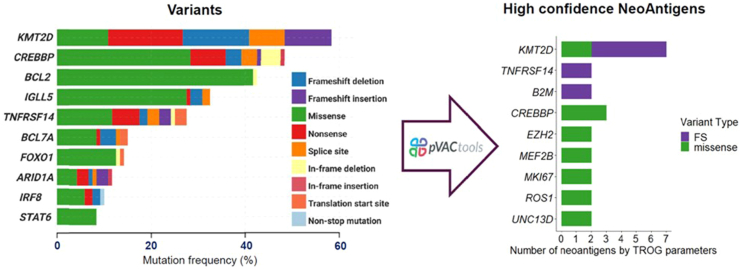
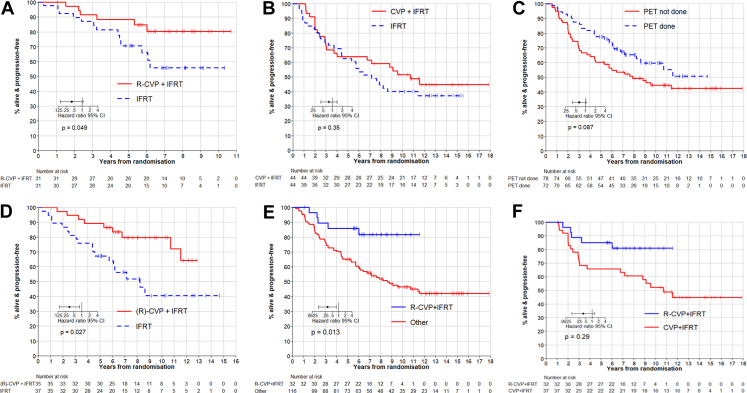
Between 2000 and 2012, 150 (75 per arm) patients were recruited. 48% were positron emission tomography (PET)-staged. By protocol, at median follow-up 11.3-years, progression-free survival (PFS) remained superior for IFRT+(R)CVP vs. IFRT (hazard ratio [HR] = 0.60, 95% CI = 0.37-0.98, p = 0.043; 10-year PFS 62% vs. 43%) respectively. Although no significant difference in overall survival was observed (HR = 0.44, 95% CI = 0.16-1.18, p = 0.11, 10-year OS 95% vs. 84%), patients receiving IFRT+(R)CVP experienced fewer composite (histological transformation and death) events (p = 0.045). PFS of IFRT + R-CVP-treated patients compared with all other treatments lacking rituximab (IFRT alone plus IFRT + CVP) was superior (HR = 0.36, 95% CI = 0.13-0.82, p = 0.013). Amongst PET-staged patients, PFS differences between IFRT + R-CVP vs. IFRT were maintained (HR = 0.38, 95% CI = 0.16-0.89, p = 0.027) indicating benefit distinct from stage migration. FL-related mutations and BCL2-translocations were not associated with PFS. However, by multivariate analysis elevated CD8A gene expression in diagnostic biopsy tissue was independently associated with improved PFS (HR = 0.45, 95% CI = 0.26-0.79, p = 0.037), a finding confirmed in both ESFL validation cohorts. CD8A gene expression was raised (p = 0.02) and CD8+ T-cell density higher within follicles in ESFL vs. advanced-stage FL (p = 0.047). Human leucocyte antigen class I specific neoantigens were detected in 43% of patients, suggesting neoantigen-specific CD8+ T-cells have a role in confining the spread of the disease.
Adjuvant R-CVP and elevated intratumoural CD8 expression were independently associated with sustained disease control after radiotherapy in ESFL.
Cancer Council Victora; National Health and Medical Research Council; Leukaemia Foundation; Mater Foundation.
我们报告了TROG99.03的长期随访结果,这是一项针对早期滤泡性淋巴瘤(ESFL)的随机III期试验,包括关于辅助性利妥昔单抗作用的新信息和转化研究。
ESFL患者被随机分为累及野放疗(IFRT)组或IFRT联合6周期环磷酰胺/长春新碱/泼尼松(IFRT + CVP)组。从2006年起,利妥昔单抗被添加到IFRT + CVP方案中(IFRT + R - CVP)。对临床和多组学参数进行了评估。研究结果在两个独立的ESFL队列(分别为99例和60例患者)中得到验证。
2000年至2012年期间,共招募了150例患者(每组75例)。48%的患者进行了正电子发射断层扫描(PET)分期。按照方案,在中位随访11.3年时,IFRT +(R)CVP组的无进展生存期(PFS)仍优于IFRT组(风险比[HR]=0.60,95%置信区间[CI]=0.37 - 0.98,p = 0.043;10年PFS分别为62%和43%)。虽然总生存期未观察到显著差异(HR = 0.44,95% CI = 0.16 - 1.18,p = 0.11,10年总生存期分别为95%和84%),但接受IFRT +(R)CVP治疗的患者发生复合事件(组织学转化和死亡)的情况较少(p = 0.045)。与所有其他未使用利妥昔单抗的治疗方案(单独IFRT加IFRT + CVP)相比,IFRT + R - CVP治疗的患者PFS更优(HR = 0.36,95% CI = 0.13 - 0.82,p = 0.013)。在PET分期的患者中,IFRT + R - CVP与IFRT之间的PFS差异依然存在(HR = 0.38,95% CI = 0.16 - 0.89,p = 0.027),表明这种获益与分期迁移无关。FL相关突变和BCL2易位与PFS无关。然而,通过多变量分析,诊断性活检组织中CD8A基因表达升高与PFS改善独立相关(HR = 0.45,95% CI = 0.26 - 0.79,p = 0.037),这一发现在两个ESFL验证队列中均得到证实。与晚期滤泡性淋巴瘤相比,ESFL患者的CD8A基因表达升高(p = 0.02),滤泡内CD8 + T细胞密度更高(p = 0.047)。43%的患者检测到人类白细胞抗原I类特异性新抗原,提示新抗原特异性CD8 + T细胞在限制疾病传播中发挥作用。
辅助性R - CVP和肿瘤内CD8表达升高与ESFL放疗后疾病的持续控制独立相关。
维多利亚癌症理事会;国家卫生与医学研究委员会;白血病基金会;马特基金会。