Zeng Dan, Zhang Jiayan, Song Zuhua, Li Qian, Zhang Dan, Li Xiaojiao, Wen Youjia, Ren Xiaofang, Wang Xinwei, Zhang Xiaodi, Tang Zhuoyue
Department of Radiology, Chongqing General Hospital, Chongqing University, Chongqing, China.
Department of Clinical and Technical Support, Philips Healthcare, Chengdu, China.
Insights Imaging. 2024 Dec 5;15(1):291. doi: 10.1186/s13244-024-01864-9.
To develop and validate a model integrating dual-layer detector spectral computed tomography (DLCT) three-dimensional (3D) volume of interest (VOI)-based quantitative parameters and clinical features for predicting Ki-67 proliferation index (PI) in pancreatic ductal adenocarcinoma (PDAC).
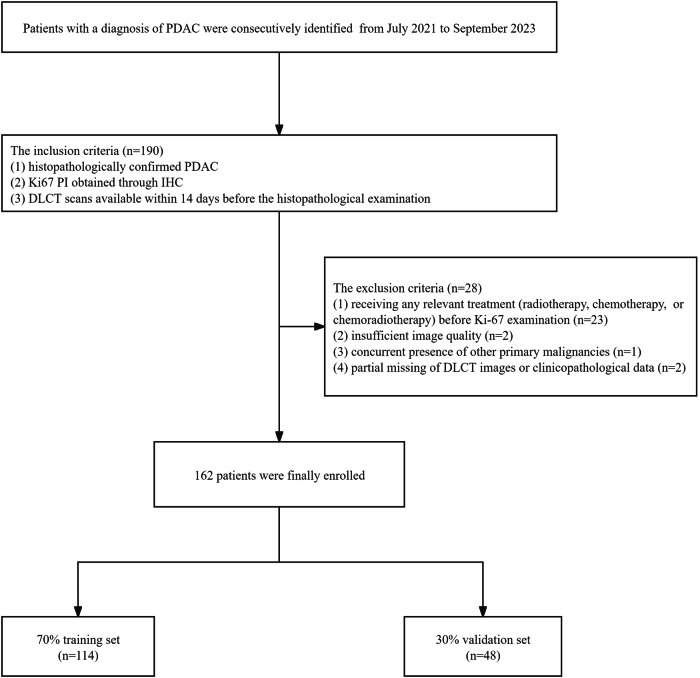
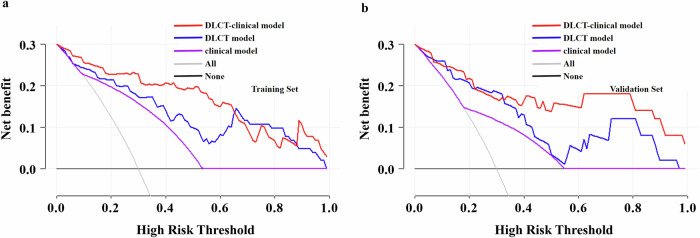
A total of 162 patients with histopathologically confirmed PDAC who underwent DLCT examination were included and allocated to the training (114) and validation (48) sets. 3D VOI-iodine concentration (IC), 3D VOI-slope of the spectral attenuation curves, and 3D VOI-effective atomic number were obtained from the portal venous phase. The significant clinical features and DLCT quantitative parameters were identified through univariate analysis and multivariate logistic regression. The discrimination capability and clinical applicability of the clinical, DLCT, and DLCT-clinical models were quantified by the Receiver Operating Characteristic curve (ROC) and Decision Curve Analysis (DCA), respectively. The optimal model was then used to develop a nomogram, with the goodness-of-fit evaluated through the calibration curve.
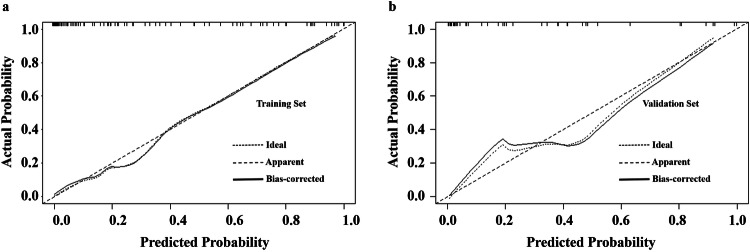
The DLCT-clinical model demonstrated superior predictive capability and a satisfactory net benefit for Ki-67 PI in PDAC compared to the clinical and DLCT models. The DLCT-clinical model integrating 3D VOI-IC and CA125 showed area under the ROC curves of 0.939 (95% CI, 0.895-0.982) and 0.915 (95% CI, 0.834-0.996) in the training and validation sets, respectively. The nomogram derived from the DLCT-clinical model exhibited favorable calibration, as depicted by the calibration curve.
The proposed model based on DLCT 3D VOI-IC and CA125 is a non-invasive and effective preoperative prediction tool demonstrating favorable predictive performance for Ki-67 PI in PDAC.
The dual-layer detector spectral computed tomography-clinical model could help predict high Ki-67 PI in pancreatic ductal adenocarcinoma patients, which may help clinicians provide appropriate and individualized treatments.
Dual-layer detector spectral CT (DLCT) could predict Ki-67 in pancreatic ductal adenocarcinoma (PDAC). The DLCT-clinical model improved the differential diagnosis of Ki-67. The nomogram showed satisfactory calibration and net benefit for discriminating Ki-67.
建立并验证一种整合双层探测器光谱计算机断层扫描(DLCT)基于三维(3D)感兴趣区(VOI)的定量参数和临床特征的模型,用于预测胰腺导管腺癌(PDAC)中的Ki-67增殖指数(PI)。
纳入162例经组织病理学确诊且接受DLCT检查的PDAC患者,并将其分为训练集(114例)和验证集(48例)。在门静脉期获取3D VOI碘浓度(IC)、3D VOI光谱衰减曲线斜率和3D VOI有效原子序数。通过单因素分析和多因素逻辑回归确定显著的临床特征和DLCT定量参数。分别通过受试者操作特征曲线(ROC)和决策曲线分析(DCA)对临床、DLCT和DLCT-临床模型的鉴别能力和临床适用性进行量化。然后使用最优模型制定列线图,并通过校准曲线评估拟合优度。
与临床和DLCT模型相比,DLCT-临床模型在预测PDAC中Ki-67 PI方面表现出卓越的预测能力和令人满意的净效益。整合3D VOI-IC和CA125的DLCT-临床模型在训练集和验证集中的ROC曲线下面积分别为0.939(95%CI,0.895-0.982)和0.915(95%CI,0.834-0.996)。如校准曲线所示,由DLCT-临床模型得出的列线图显示出良好的校准。
所提出的基于DLCT 3D VOI-IC和CA125的模型是一种无创且有效的术前预测工具,对PDAC中的Ki-67 PI具有良好的预测性能。
双层探测器光谱计算机断层扫描-临床模型有助于预测胰腺导管腺癌患者的高Ki-67 PI,这可能有助于临床医生提供适当的个体化治疗。
双层探测器光谱CT(DLCT)可预测胰腺导管腺癌(PDAC)中的Ki-67。DLCT-临床模型改善了对Ki-67的鉴别诊断。列线图在鉴别Ki-67方面显示出令人满意的校准和净效益。