Balingit April Keith, Grande Phoebe Grace, Nicolasora Amalea Dulcene, Polotan Francisco Gerardo, Pantoni Roslind Anne, Abulencia Miguel Francisco, Chu Maria Yna Joyce, Rivera Nicole, Oblepias Marie Socouer, Garcia Jemelyn
Research Institute for Tropical Medicine, Muntinlupa, Philippines.
Front Public Health. 2024 Nov 21;12:1387636. doi: 10.3389/fpubh.2024.1387636. eCollection 2024.
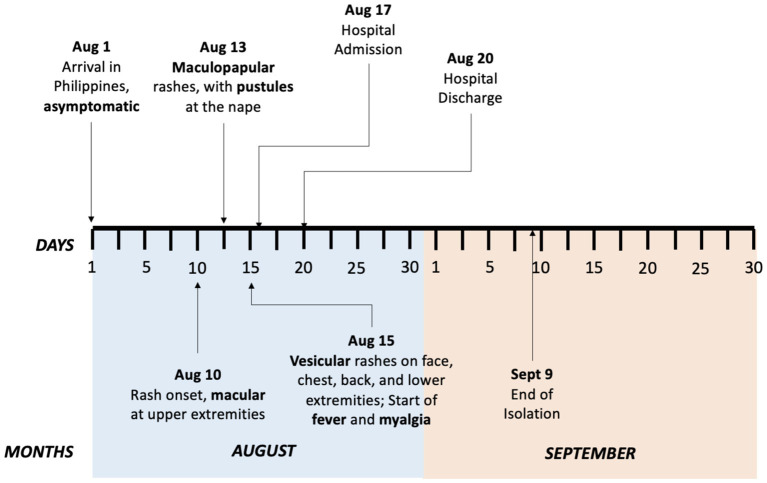
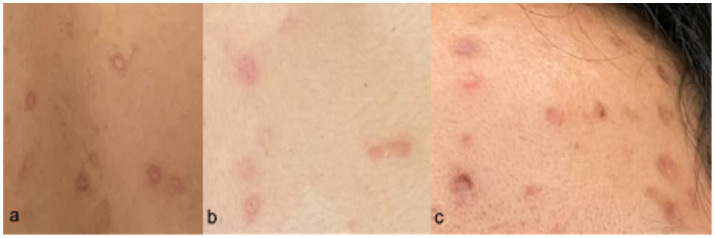
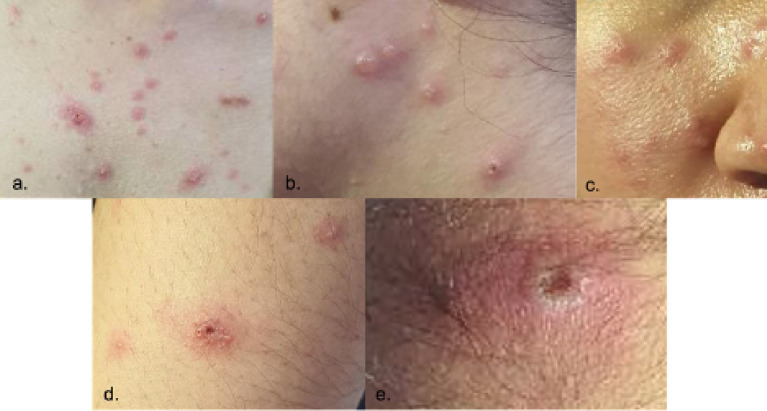
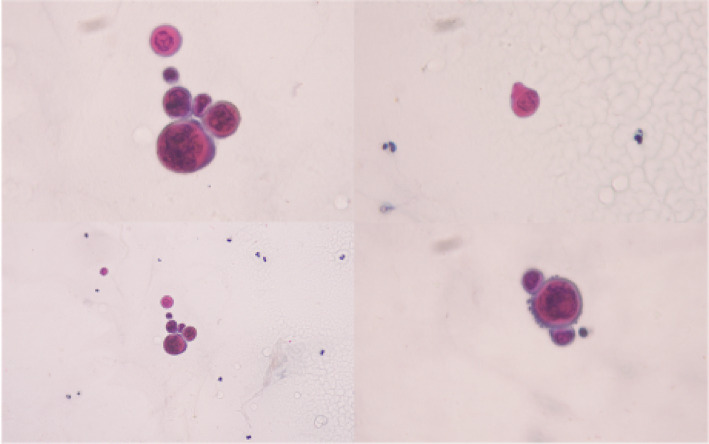
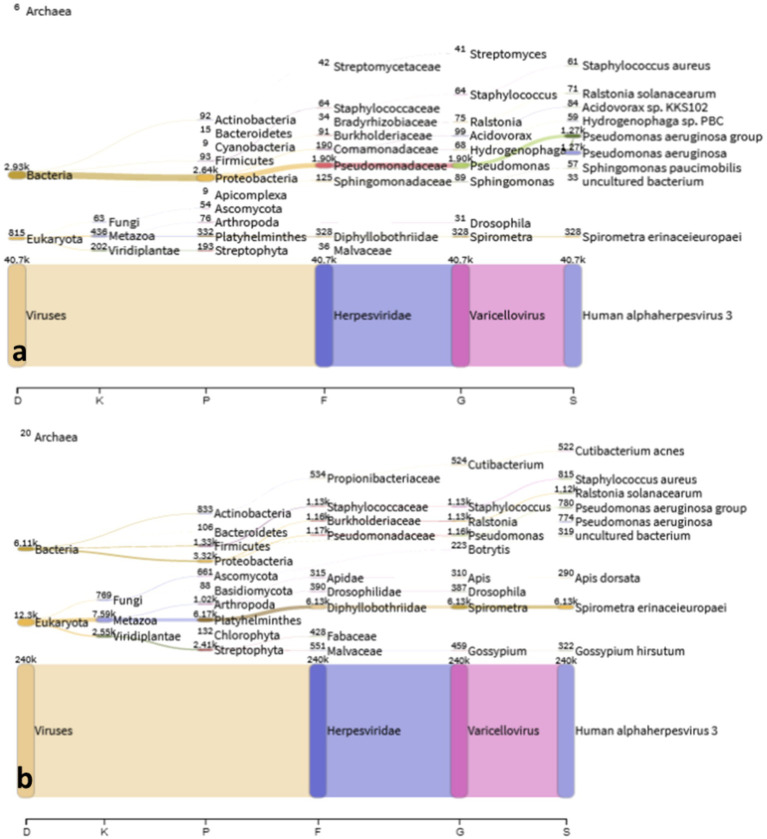
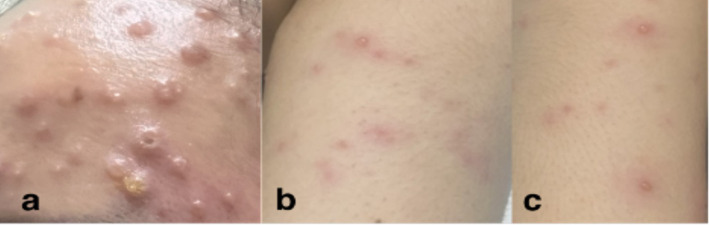
We report the first travel-related case of a possible Mpox-Varicella zoster virus (VZV) co-infection in the Philippines, a country that is endemic for Varicella but non-endemic for Mpox. A 29-year-old Filipino, female, with a travel history to Switzerland and with no prior history of VZV infection sought consultation due to rashes. She presented with multiple papular, pustular, and vesicular skin lesions, some with umbilication and with irregular borders, on the face, neck, trunk, inguinal area, upper extremities, and right leg. She also had bilateral submandibular and post-auricular lymphadenopathies. Tzanck smear exhibited viral cytopathic effects. She tested positive for Mpox infection (Clade II) and Varicella infection via quantitative real-time polymerase chain reaction (qPCR) tests but with a high CT value obtained from the Mpox PCR. Shotgun metagenomic sequencing (mNGS) successfully recovered sequences from the Varicella zoster virus which corroborated with the high viral load detected using qPCR. In contrast, shotgun mNGS was not able to generate a Mpox consensus sequence due to very few reads mapped to the Mpox virus reference sequence, which raised the question if there was the presence of a true Mpox-Varicella co-infection in our patient. Nevertheless, systemic and topical acyclovir was given to the patient. She was discharged and continued home isolation for 30 days from the rash onset. Strategies have been formed by the country's healthcare facilities to properly identify Mpox infection. However, Mpox co-infection with other viral diseases presented a challenge in the proper diagnosis of our patient. This prompted a high index of suspicion and the usage of suitable diagnostic tests. With proper clinical evaluation and utilization of appropriate diagnostic tests, we were able to diagnose the first Filipino patient with a possible Mpox and Varicella zoster virus co-infection.
我们报告了菲律宾首例与旅行相关的可能的猴痘-水痘带状疱疹病毒(VZV)合并感染病例,该国水痘为地方病,但猴痘并非地方病。一名29岁的菲律宾女性,有前往瑞士的旅行史,既往无VZV感染史,因皮疹前来咨询。她面部、颈部、躯干、腹股沟区、上肢和右腿出现多处丘疹、脓疱和水疱性皮肤损害,部分有脐凹和不规则边界。她还伴有双侧颌下和耳后淋巴结病。Tzanck涂片显示病毒细胞病变效应。通过定量实时聚合酶链反应(qPCR)检测,她的猴痘感染(II型分支)和水痘感染均呈阳性,但猴痘PCR检测的CT值较高。鸟枪法宏基因组测序(mNGS)成功从水痘带状疱疹病毒中获得序列,这与使用qPCR检测到的高病毒载量相符。相比之下,由于映射到猴痘病毒参考序列的读段极少,鸟枪法mNGS未能生成猴痘一致序列,这引发了我们的患者是否存在真正的猴痘-水痘合并感染的疑问。尽管如此,仍给患者使用了全身性和局部性阿昔洛韦。她已出院,并从皮疹出现开始继续居家隔离30天。该国医疗机构已制定策略以正确识别猴痘感染。然而,猴痘与其他病毒性疾病的合并感染给我们患者的正确诊断带来了挑战。这促使我们高度怀疑并使用合适的诊断测试。通过适当的临床评估和使用适当的诊断测试,我们得以诊断出首例可能合并猴痘和水痘带状疱疹病毒感染的菲律宾患者。