Tsumuki Yuto, Kawamata Hirofumi, Hori Masatoshi, Shako Daiki, Kawasaki Tatsuya
Department of Cardiology, Matsushita Memorial Hospital, Moriguchi, JPN.
Department of Emergency Medicine, Matsushita Memorial Hospital, Moriguchi, JPN.
Cureus. 2024 Nov 4;16(11):e73015. doi: 10.7759/cureus.73015. eCollection 2024 Nov.
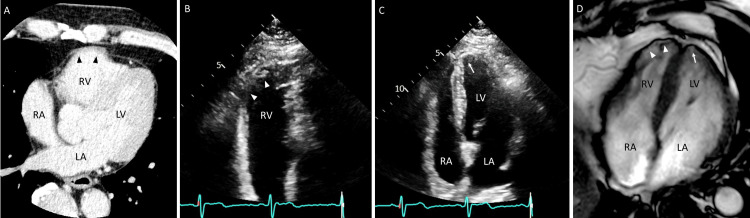
Sarcoidosis has a heterogeneous clinical presentation and remains difficult to diagnose, especially in isolated cardiac sarcoidosis (CS). We report a case of life-threatening arrhythmia that led to the diagnosis of isolated CS. A 63-year-old man presented with sustained ventricular tachycardia that was thought to originate from the anterolateral free wall of the right ventricle. Electrocardiography, echocardiography, and coronary computed tomography performed after the return to sinus rhythm were initially considered unremarkable, but right ventricular free wall bulging was later noted on computed tomography. Follow-up echocardiography revealed abnormal wall motion not only in the right ventricular free wall but also in the left ventricular apex. The patient was finally diagnosed with isolated CS and was scheduled for steroid treatment after receiving an implantable cardioverter-defibrillator.
结节病临床表现多样,诊断困难,尤其是孤立性心脏结节病(CS)。我们报告一例危及生命的心律失常导致孤立性CS诊断的病例。一名63岁男性出现持续性室性心动过速,推测起源于右心室前外侧游离壁。恢复窦性心律后进行的心电图、超声心动图和冠状动脉计算机断层扫描最初被认为无异常,但后来计算机断层扫描发现右心室游离壁膨出。随访超声心动图显示不仅右心室游离壁,而且左心室心尖部的壁运动异常。该患者最终被诊断为孤立性CS,在植入植入式心律转复除颤器后计划接受类固醇治疗。