Neferu Ramona, Fleck Rebecca
Department of Medicine, McMaster University, Hamilton, Ontario, Canada
Parkwood Hospital, London, Ontario, Canada.
BMJ Open Qual. 2024 Dec 7;13(4):e002915. doi: 10.1136/bmjoq-2024-002915.
Acquired brain injury (ABI) is a major cause of disability. Timely access to inpatient ABI rehabilitation is associated with improved outcomes at the patient, system, and societal levels.
Wait times to access the inpatient ABI rehabilitation programme at the local regional rehabilitation centre by patients referred from community hospitals were consistently greater than provincial targets and benchmarks.
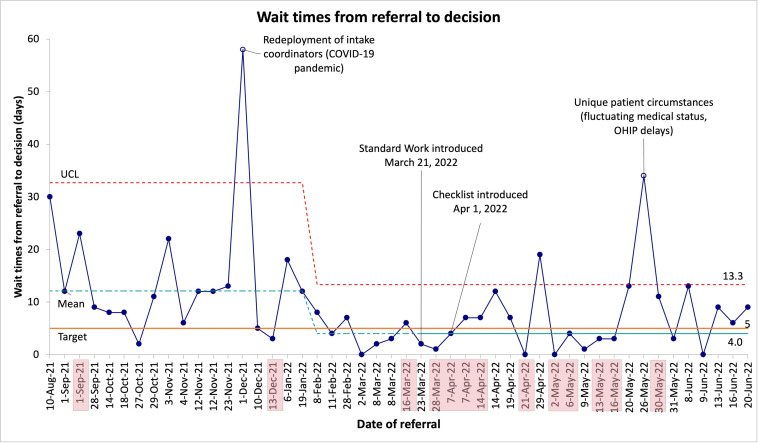
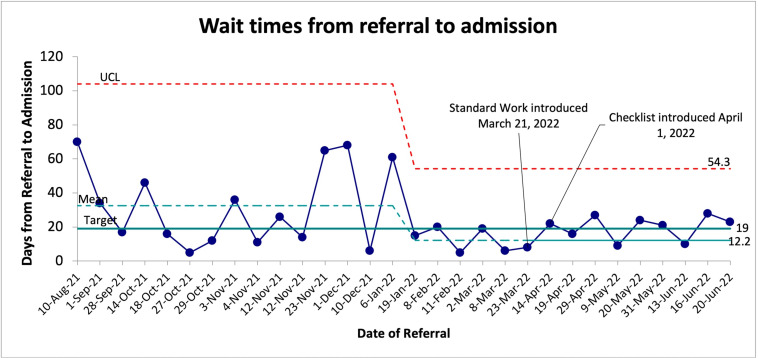
This initiative aimed to reduce the mean wait times from referral to admission by 30% (from 27 to 19 days) during the 12-month project period. The secondary aim was to concurrently achieve a reduction in the mean wait times for decisions from 9.5 to 5 days during the same period.
A non-randomised time-series design was undertaken. Baseline and postintervention wait times were obtained from patient intake charts. Process mapping, value analysis and five-why analysis were used to identify root causes for delays in the intake process. Referring hospital staff and the ABI Rehab interdisciplinary team members were engaged in change idea development and refinement. Iterative Plan-Do-Study-Act cycles were used to improve the change ideas' usability and uptake. Data analysis was performed using the QI Macros package in Microsoft Excel.
Root causes for delays included frequent incomplete referrals, variability in the intake process and limitations in rehab bed availability. Two change ideas were introduced: (1) a standardised intake protocol and (2) a referral checklist. Within 3 months, the mean decision wait times were reduced to 4 days (58% reduction), and the mean admission wait times were reduced to 12 days (54% reduction).
This initiative led to the systematic standardisation of the intake process for the local regional ABI rehab programme. Wait time improvements surpassing the initial aims were observed and may inform future benchmarks.
后天性脑损伤(ABI)是导致残疾的主要原因。及时接受住院ABI康复治疗与患者、系统和社会层面的更好预后相关。
社区医院转诊的患者在当地地区康复中心接受住院ABI康复项目的等待时间一直超过省级目标和基准。
该倡议旨在在12个月的项目期内将从转诊到入院的平均等待时间减少30%(从27天降至19天)。次要目标是在同一时期内将决策的平均等待时间从9.5天降至5天。
采用非随机时间序列设计。从患者入院图表中获取基线和干预后的等待时间。通过流程映射、价值分析和五个为什么分析来确定入院流程延迟的根本原因。转诊医院工作人员和ABI康复跨学科团队成员参与了变革想法的开发和完善。采用迭代的计划-执行-研究-行动循环来提高变革想法的可用性和接受度。使用Microsoft Excel中的QI Macros软件包进行数据分析。
延迟的根本原因包括频繁的转诊不完整、入院流程的 variability以及康复床位可用性的限制。引入了两个变革想法:(1)标准化入院协议和(2)转诊清单。在3个月内,决策的平均等待时间降至4天(减少了58%),入院的平均等待时间降至12天(减少了54%)。
该倡议导致当地地区ABI康复项目入院流程的系统标准化。观察到等待时间的改善超过了最初目标,这可能为未来的基准提供参考。