Jeyashree Kathiresan, Thangaraj Jeromie W V, Shanmugasundaram Devika, Giridharan Sri Lakshmi Priya, Pandey Sumit, Shanmugasundaram Prema, Ramasamy Sabarinathan, Janagaraj Venkateshprabhu, Arunachalam Sivavallinathan, Sharma Rahul, Shah Vaibhav, Bagepally Bhavani Shankara, Chadwick Joshua, Shewade Hemant Deepak, Chowdhury Aniket, Iyer Swati, Rao Raghuram, Mattoo Sanjay K, Murhekar Manoj V
ICMR-National Institute of Epidemiology (ICMR-NIE), R-127, TNHB, Ayapakkam, Chennai, Tamil Nadu, 600077, India.
TB Support Network, WHO Country Office for India, New Delhi, India.
Glob Health Res Policy. 2024 Dec 9;9(1):51. doi: 10.1186/s41256-024-00392-9.
Tuberculosis (TB) poses a significant social and economic burden to households of persons with TB (PwTB). Despite free diagnosis and care under the National TB Elimination Programme (NTEP), individuals often experience significant out-of-pocket expenditure and lost productivity, causing financial catastrophe. We estimated the costs incurred by the PwTB during TB care and identified the factors associated with the costs.
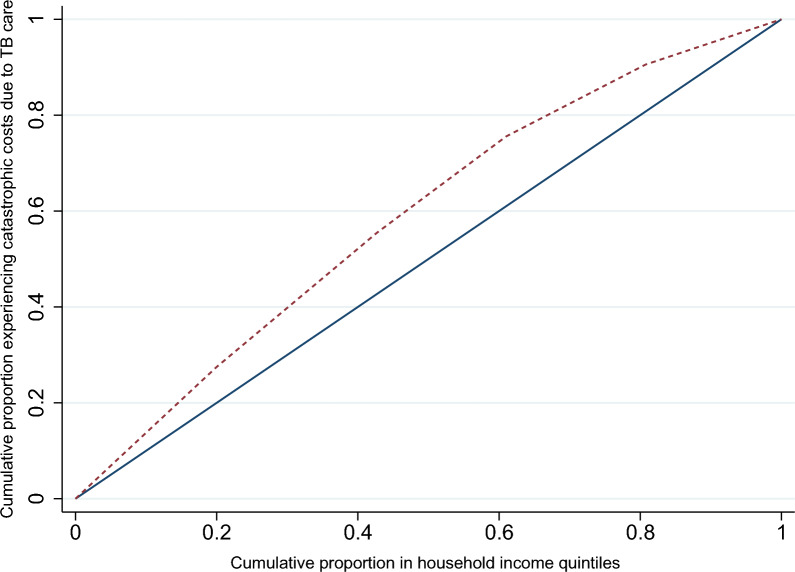
In our cross-sectional study, we used multi-stage sampling to select PwTB notified under the NTEP, whose treatment outcome was declared between May 2022 and February 2023. Total patient costs were measured through direct medical, non-medical and indirect costs. Catastrophic costs were defined as expenditure on TB care > 20% of the annual household income. We determined the factors influencing the total cost of TB care using median regression. We plotted concentration curves to depict the equity in distribution of catastrophic costs across income quintiles. We used a cluster-adjusted, generalized model to determine the factors associated with catastrophic costs.
The mean (SD) age of the 1407 PwTB interviewed was 40.8 (16.8) years. Among them, 865 (61.5%) were male, and 786 (55.9%) were economically active. Thirty-four (2.4%) had Drug Resistant TB (DRTB), and 258 (18.3%) had been hospitalized for TB. The median (Interquartile range [IQR] and 95% confidence interval [CI]) of total costs of TB care was US$386.1 (130.8, 876.9). Direct costs accounted for 34% of the total costs, with a median of US$78.4 (43.3, 153.6), while indirect costs had a median of US$279.8 (18.9,699.4). PwTB < 60 years of age (US$446.1; 370.4, 521.8), without health insurance (US$464.2; 386.7, 541.6), and those hospitalized(US$900.4; 700.2, 1100.6) for TB experienced higher median costs. Catastrophic costs, experienced by 45% of PwTB, followed a pro-poor distribution. Hospitalized PwTB (adjusted prevalence ratio [aPR] = 1.9; 1.6, 2.2) and those notified from the private sector (aPR = 1.4; 1.1, 1.8) were more likely to incur catastrophic costs.
PwTB in India incur high costs mainly due to lost productivity and hospitalization. Nearly half of them experience catastrophic costs, especially those from poorer economic quintiles. Enabling early notification of TB, expanding the coverage of health insurance schemes to include PwTB, and implementing TB sensitive strategies to address social determinants of TB may significantly reduce catastrophic costs incurred by PwTB.
结核病给结核病患者家庭带来了巨大的社会和经济负担。尽管根据国家结核病消除计划(NTEP)可享受免费诊断和治疗,但患者个人仍经常面临大量自付费用和生产力损失,导致经济灾难。我们估计了结核病患者在结核病治疗期间产生的费用,并确定了与这些费用相关的因素。
在我们的横断面研究中,我们采用多阶段抽样方法选择在NTEP下通报的结核病患者,其治疗结果于2022年5月至2023年2月期间公布。通过直接医疗、非医疗和间接成本来衡量患者的总费用。灾难性成本定义为结核病治疗支出超过家庭年收入的20%。我们使用中位数回归来确定影响结核病治疗总成本的因素。我们绘制了集中曲线,以描述灾难性成本在收入五分位数中的公平分配情况。我们使用聚类调整的广义模型来确定与灾难性成本相关的因素。
接受访谈的1407名结核病患者的平均(标准差)年龄为40.8(16.8)岁。其中,865名(61.5%)为男性,786名(55.9%)有经济活动能力。34名(2.4%)患有耐多药结核病(DRTB),258名(18.3%)因结核病住院治疗。结核病治疗总费用的中位数(四分位间距[IQR]和95%置信区间[CI])为386.1美元(130.8,876.9)。直接成本占总成本的34%,中位数为78.4美元(43.3,153.6),而间接成本的中位数为279.8美元(18.9,699.4)。年龄小于60岁的结核病患者(446.1美元;370.4,521.8)、没有医疗保险的患者(464.2美元;386.7,541.6)以及因结核病住院治疗的患者(900.4美元;700.2,1100.6)的费用中位数较高。45%的结核病患者经历了灾难性成本,呈有利于穷人的分布。因结核病住院治疗的患者(调整后患病率比[aPR]=1.9;1.6,2.2)和来自私营部门通报的患者(aPR=1.4;1.1,1.8)更有可能产生灾难性成本。
印度的结核病患者产生高昂费用主要是由于生产力损失和住院治疗。近一半的患者经历了灾难性成本,尤其是来自经济较贫困五分位数的患者。实现结核病的早期通报、扩大医疗保险计划的覆盖范围以纳入结核病患者,以及实施针对结核病社会决定因素的结核病敏感策略,可能会显著降低结核病患者产生的灾难性成本。