Department of Community Medicine, Government Medical College Bhavnagar (Maharaja Krishnakumarsinhji Bhavnagar University), Near ST Bus Stand, Jail Road, Bhavnagar, Gujarat 364001, India.
Division of Pulmonary and Critical Care Medicine and Center for Tuberculosis, University of California San Francisco (UCSF), California, USA.
Infect Dis Poverty. 2020 Oct 19;9(1):144. doi: 10.1186/s40249-020-00760-w.
India reports the highest number of tuberculosis (TB) cases worldwide. Poverty has a dual impact as it increases the risk of TB and exposes the poor to economic hardship when they develop TB. Our objective was to estimate the costs incurred by patients with drug-susceptible TB in Bhavnagar (western India) using an adapted World Health Organization costing tool.
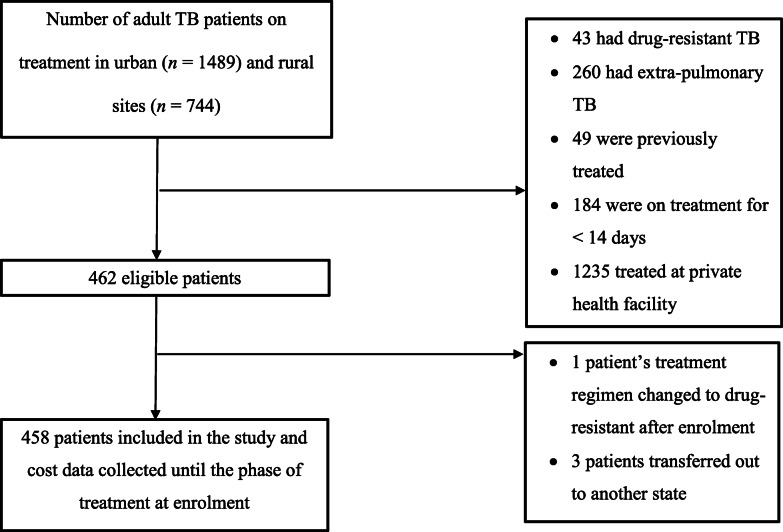
We conducted a descriptive cross-sectional study of adults, notified in the public sector and being treated for drug-susceptible pulmonary TB during January-June 2019, in six urban and three rural blocks of Bhavnagar region, Gujarat state, India. The direct and indirect TB-related costs, as well as patients' coping strategies, were assessed for the overall care of TB till treatment completion. Catastrophic costs were defined as total costs > 20% of annual household income (excluding any amount received from cash transfer programs or borrowed). Median and interquartile range (IQR) was used to summarize patient costs. The median costs between any two groups were compared using the median test. The association between any two categorical variables was tested by the Pearson chi-squared test. All costs were described in US dollars (USD). During the study period, on average, one USD equalled 70 Indian Rupees.
Of 458 patients included, 70% were male, 62% had no formal education, 71% lived in urban areas, and 96% completed TB treatment. The median (IQR) total costs were USD 8 (5-28), direct medical costs were USD 0 (0-0), direct non-medical costs were USD 3 (2-4) and indirect costs were USD 6 (3-13). Among direct non-medical costs, travel cost (median = USD 3, IQR: 2-4) to attend health facilities were the most prominent, whereas the indirect costs were mainly contributed by the patient's loss of wages (median = USD 3, IQR: 0-6). Four percent of patients faced catastrophic costs, 11% borrowed money to cover costs and 7% lost their employment; the median working days lost to TB was 30 (IQR: 15-45). A majority (88%) of patients received a median USD 43 (IQR: 41-43) as part of a cash transfer program for TB patients.
Treatment completion was high and the costs incurred by TB patients were low in this setting. However, negative financial consequences occur even in low-cost settings. The role of universal cash transfer programs in such settings requires further study.
印度报告的结核病(TB)病例数居世界首位。贫困具有双重影响,它不仅增加了患结核病的风险,而且当穷人患上结核病时,还使他们面临经济困难。我们的目的是使用世界卫生组织(WHO)成本核算工具,估算印度西部巴夫那加尔(Bhavnagar)地区耐多药结核病(TB)患者的费用。
我们对 2019 年 1 月至 6 月期间在古吉拉特邦巴夫那加尔地区六个城市和三个农村街区公共部门报告并正在接受耐多药肺结核治疗的成年人进行了描述性横断面研究。评估了直接和间接与结核病相关的成本,以及患者在结核病治疗完成前的所有治疗过程中的应对策略。灾难性费用定义为总费用超过家庭年收入的 20%(不包括从现金转移计划收到或借款的任何金额)。使用中位数和四分位距(IQR)来总结患者的费用。使用中位数检验比较任何两组之间的中位数成本。使用皮尔逊卡方检验测试任何两个分类变量之间的关联。所有费用均以美元(USD)表示。在研究期间,平均一美元等于 70 印度卢比。
在 458 名患者中,70%为男性,62%没有接受过正规教育,71%居住在城市地区,96%完成了结核病治疗。总费用中位数(IQR)为 8 美元(5-28),直接医疗费用为 0 美元(0-0),直接非医疗费用为 3 美元(2-4),间接费用为 6 美元(3-13)。在直接非医疗费用中,前往医疗机构的交通费用(中位数=3 美元,IQR:2-4)最为突出,而间接费用主要是患者的工资损失(中位数=3 美元,IQR:0-6)。4%的患者面临灾难性费用,11%借钱支付费用,7%失业;因结核病而损失的工作天数中位数为 30 天(IQR:15-45)。大多数(88%)患者获得了结核病患者现金转移计划的 43 美元(IQR:41-43)。
在该环境中,治疗完成率较高,结核病患者的费用较低。然而,即使在低成本环境中也会产生负面的经济后果。在这种情况下,普遍的现金转移计划的作用需要进一步研究。