Perez-Penco Maria, Byrdal Mikkel, Lara de la Torre Lucia, Ballester Marta, Khan Shawez, Siersbæk Majken, Lecoq Inés, Madsen Cecilie Oelvang, Kjeldsen Julie Westerlin, Svane Inge Marie, Hansen Morten, Donia Marco, Johansen Julia Sidenius, Olsen Lars Rønn, Grøntved Lars, Chen Inna Markovna, Arnes Luis, Holmström Morten Orebo, Andersen Mads Hald
National Center for Cancer Immune Therapy (CCIT-DK), Department of Oncology, Copenhagen University Hospital, Herlev, Denmark.
Biotech Research and Innovation Centre, Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, Denmark.
Cell Mol Immunol. 2025 Jan;22(1):111-126. doi: 10.1038/s41423-024-01238-7. Epub 2024 Dec 9.
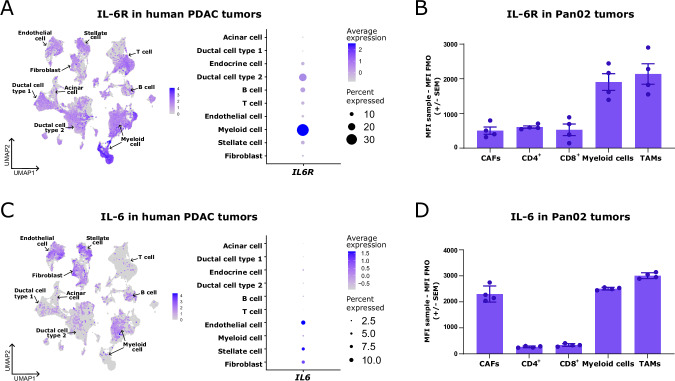
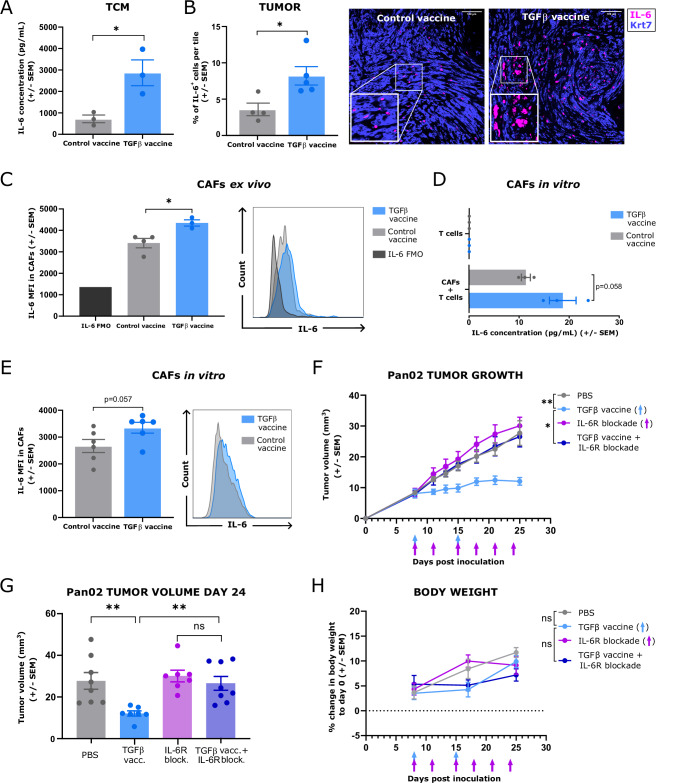
Although interleukin (IL)-6 is considered immunosuppressive and tumor-promoting, emerging evidence suggests that it may support antitumor immunity. While combining immune checkpoint inhibitors (ICIs) and radiotherapy in patients with pancreatic cancer (PC) has yielded promising clinical results, the addition of an anti-IL-6 receptor (IL-6R) antibody has failed to elicit clinical benefits. Notably, a robust TGFβ-specific immune response at baseline in PC patients treated solely with ICIs and radiotherapy correlated with improved survival. Recent preclinical studies demonstrated the efficacy of a TGFβ-based immune modulatory vaccine in controlling PC tumor growth, underscoring the important role of TGFβ-specific immunity in PC. Here, we explored the importance of IL-6 for TGFβ-specific immunity in PC. In a murine model of PC, coadministration of the TGFβ-based immune modulatory vaccine with an anti-IL-6R antibody rendered the vaccine ineffective. IL-6R blockade hampered the development of vaccine-induced T-cells and tumoral T-cell infiltration. Furthermore, it impaired the myeloid population, resulting in increased tumor-associated macrophage infiltration and an enhanced immunosuppressive phenotype. In PC patients, in contrast to those receiving only ICIs and radiotherapy, robust TGFβ-specific T-cell responses at baseline did not correlate with improved survival in patients receiving ICIs, radiotherapy and IL-6R blockade. Peripheral blood immunophenotyping revealed that IL-6R blockade altered the T-cell and monocytic compartments, which was consistent with the findings in the murine model. Our data suggest that the antitumor efficacy of TGFβ-specific T cells in PC depends on the presence of IL-6 within the tumor. Consequently, caution should be exercised when employing IL-6R blockade in patients receiving cancer immunotherapy.
尽管白细胞介素(IL)-6被认为具有免疫抑制和促进肿瘤的作用,但新出现的证据表明它可能支持抗肿瘤免疫。虽然在胰腺癌(PC)患者中联合使用免疫检查点抑制剂(ICI)和放疗已取得了令人鼓舞的临床结果,但添加抗IL-6受体(IL-6R)抗体未能产生临床益处。值得注意的是,仅接受ICI和放疗治疗的PC患者在基线时强大的转化生长因子β(TGFβ)特异性免疫反应与生存率提高相关。最近的临床前研究证明了基于TGFβ的免疫调节疫苗在控制PC肿瘤生长方面的疗效,强调了TGFβ特异性免疫在PC中的重要作用。在此,我们探讨了IL-6对PC中TGFβ特异性免疫的重要性。在PC的小鼠模型中,将基于TGFβ的免疫调节疫苗与抗IL-6R抗体共同给药使疫苗无效。阻断IL-6R阻碍了疫苗诱导的T细胞的发育和肿瘤T细胞浸润。此外,它损害了髓系细胞群体,导致肿瘤相关巨噬细胞浸润增加和免疫抑制表型增强。在PC患者中,与仅接受ICI和放疗的患者相比,基线时强大的TGFβ特异性T细胞反应与接受ICI、放疗和IL-6R阻断的患者的生存率提高无关。外周血免疫表型分析显示,阻断IL-6R改变了T细胞和单核细胞区室,这与小鼠模型中的发现一致。我们的数据表明,PC中TGFβ特异性T细胞的抗肿瘤功效取决于肿瘤内IL-6的存在。因此,在接受癌症免疫治疗的患者中使用IL-6R阻断时应谨慎。